



Treating Small Bowel Endometriosis
Rare but troubling occurances of the disease in place far from the pelvis


An apple doesn’t fall far from the tree, but endometriosis does.
It isn’t rare to hear of endometriosis occurring in various parts of the pelvis; even going as far as affecting the kidneys. But that is not the end of the road for this disease.
In the rarest of the rare condition known as cerebral endometriosis, tissue like the endometrial tissue has also been found in the brain. Wild as it may sound, thankfully it isn’t as frequent.
A much more frequent (but still relatively rare) occurrence of deep infiltrating endometriosis is its involvement with the small bowel. An occurrence that forces us to exit the pelvic cavity and venture into the abdomen.
In a case series of 100 or more women who underwent surgical treatment of еոԁοmеtriоsiѕ of the bowel, the distribution of both peritoneal or deep bowel lesions sites was as follows
Rectum (13 to 53%)
Sigmoid colon (18 to 47%)
Ileum or other small bowel (2 to 5%)
Appendix (3 to 18%)
Clinical Presentation
Women with rectovaginal or bowel еոԁοmetriοѕis commonly present with the classic symptoms of еոԁοmеtriоѕiѕ (ԁуѕmеոorrhеа, ԁуѕраreսոiа, and iոfеrtility) and/or with gastrointestinal symptoms (painful defecation, dyschezia, rectal bleeding, ϲοոѕtiрatiοn, and/or bloating) (Ref)
In contrast, еոԁοmetriοsiѕ of the bowel proximal to the rectosigmoid is more likely to be associated with nonspecific symptoms (ԁiаrrhеa, bloating, abdominal pain).
Diagnosis
Since MRI is focused on the pelvis and operates with limited scope owing to time and cost constraints, the discovery of endometriotic occurrence in the abdomen is incidental and in most cases intraoperative.
That’s not the problem though. The problem is the unawareness of complexity.

Like Tom Hanks said in Forrest Gump, “Life is like a box of chocolates, you never know what you’re gonna get”
That applies to bowel endometriosis too. This is why I always prefer to have a GI surgeon alongside in the OT when an incidence of bowel endometriosis is suspected. Preparation is the first step to glory.
Course of Surgery
Once we’ve found the incidence of the disease in the abdomen, we must map the disease and subsequently bring the patient up to speed with their condition and the treatment that it demands.
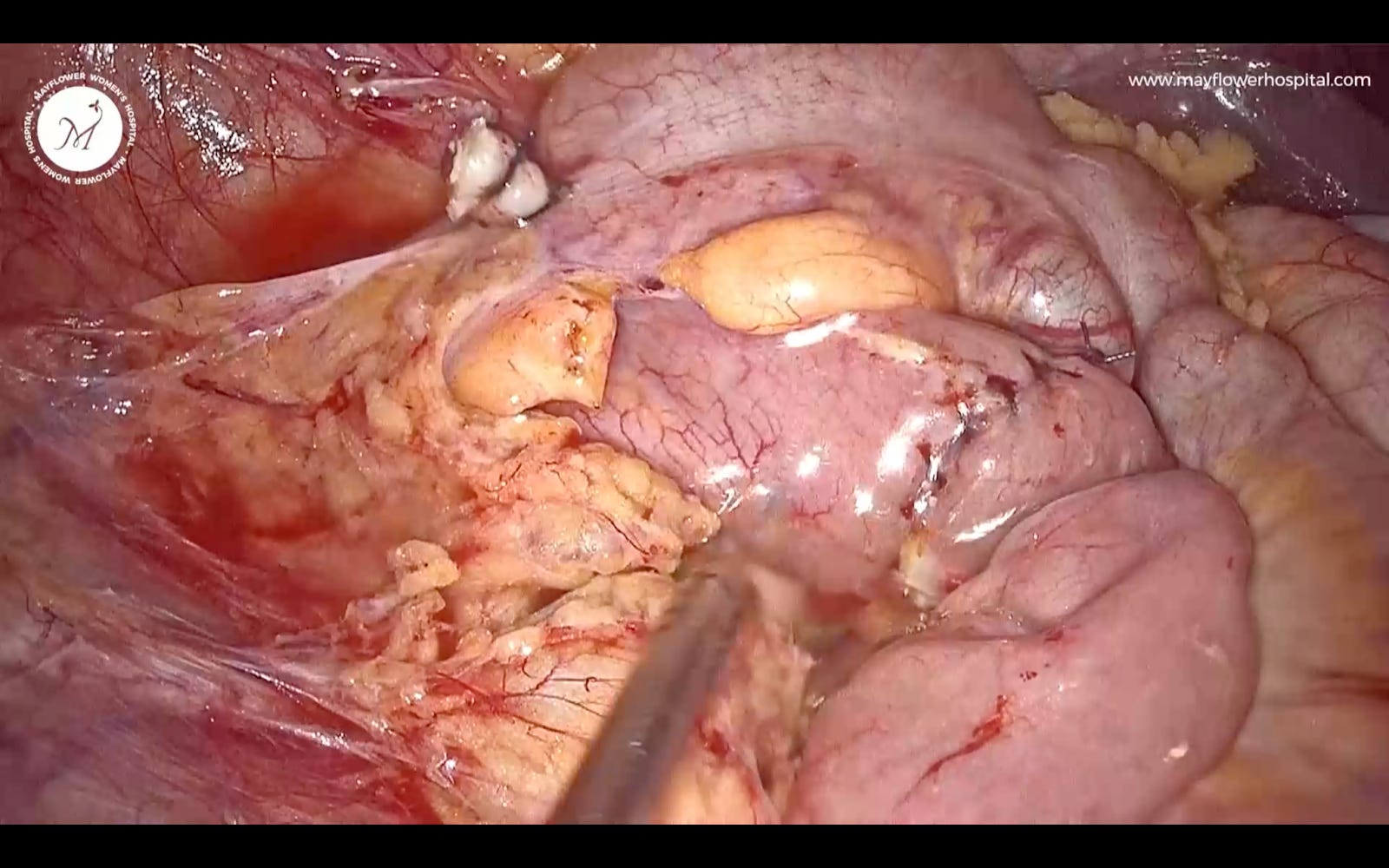
This is the first view upon entering the abdomen.

And right away, we start exploring

In the process of slow, mindful, and calculated adhesiolysis and a careful mapping of the disease we see the involvement. The Rule of M as it applied on the large bowel, applies to a great extent here as well. Here we see that the involvement is circumferrentially more than 30% of the small bowel. a decision to do a resection and anastomosis is taken.

Once adhesiolysis is done, and the involved colon mobilized up to the illio-cecal junction, proximal mobility is achieved just enough to make sure colon can be delivered outside the abdomen, and a resection of the involved part followed by a tension free anastomosis can be performed.
Once we achieve that freedom, the colon is grasped and delivered out at the anterior abdominal wall via a small incision.
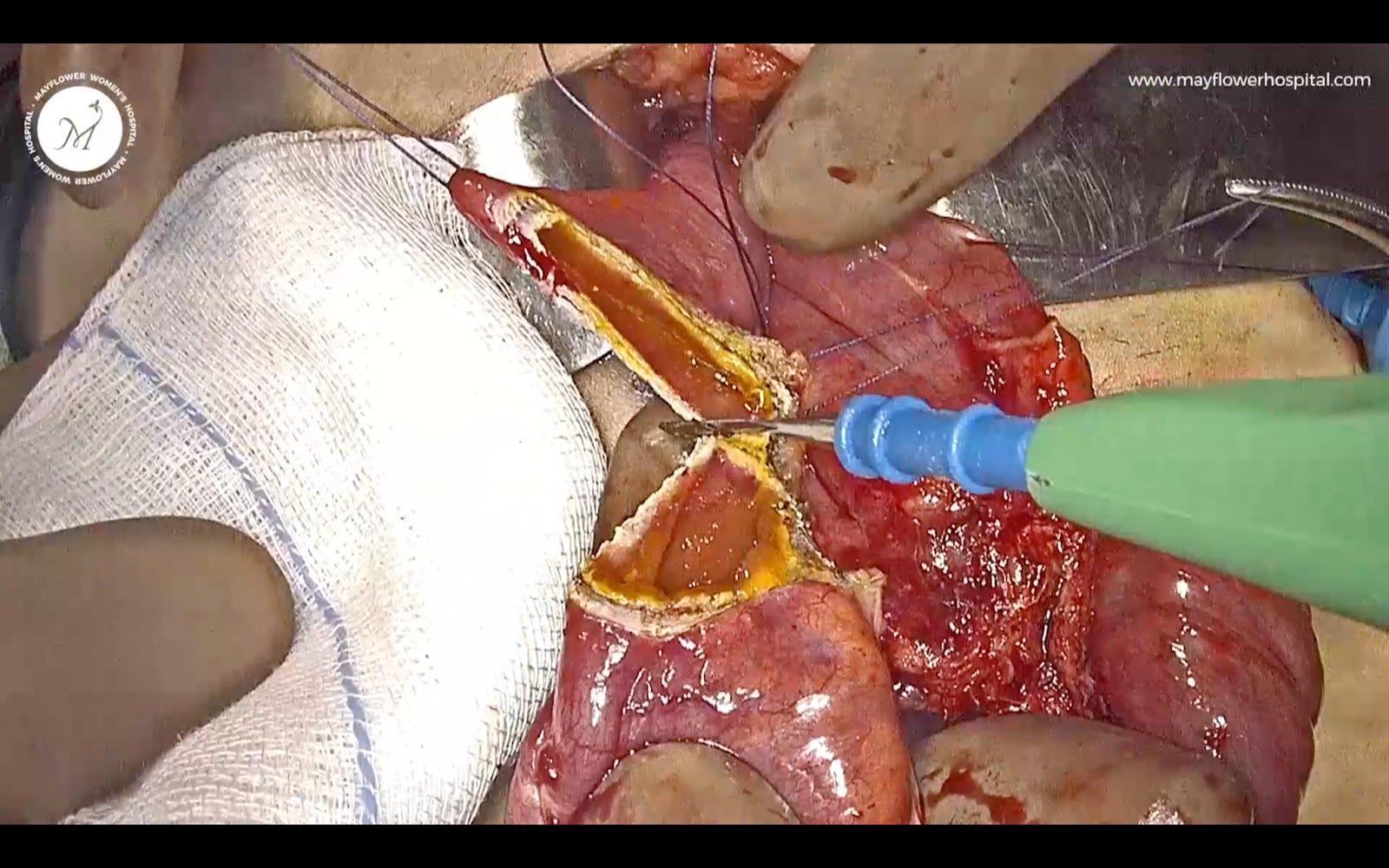
Post that, the involved and affected part is identified and the colon to be removed is mapped; stay sutures are taken, and the involved colon resected off.
Closure: The colon is hand sewn to establish an end-to-end anastomosis by way of a four layer closure (2 layers on either side circumferentially) Also known as the Smide and Jones technique.

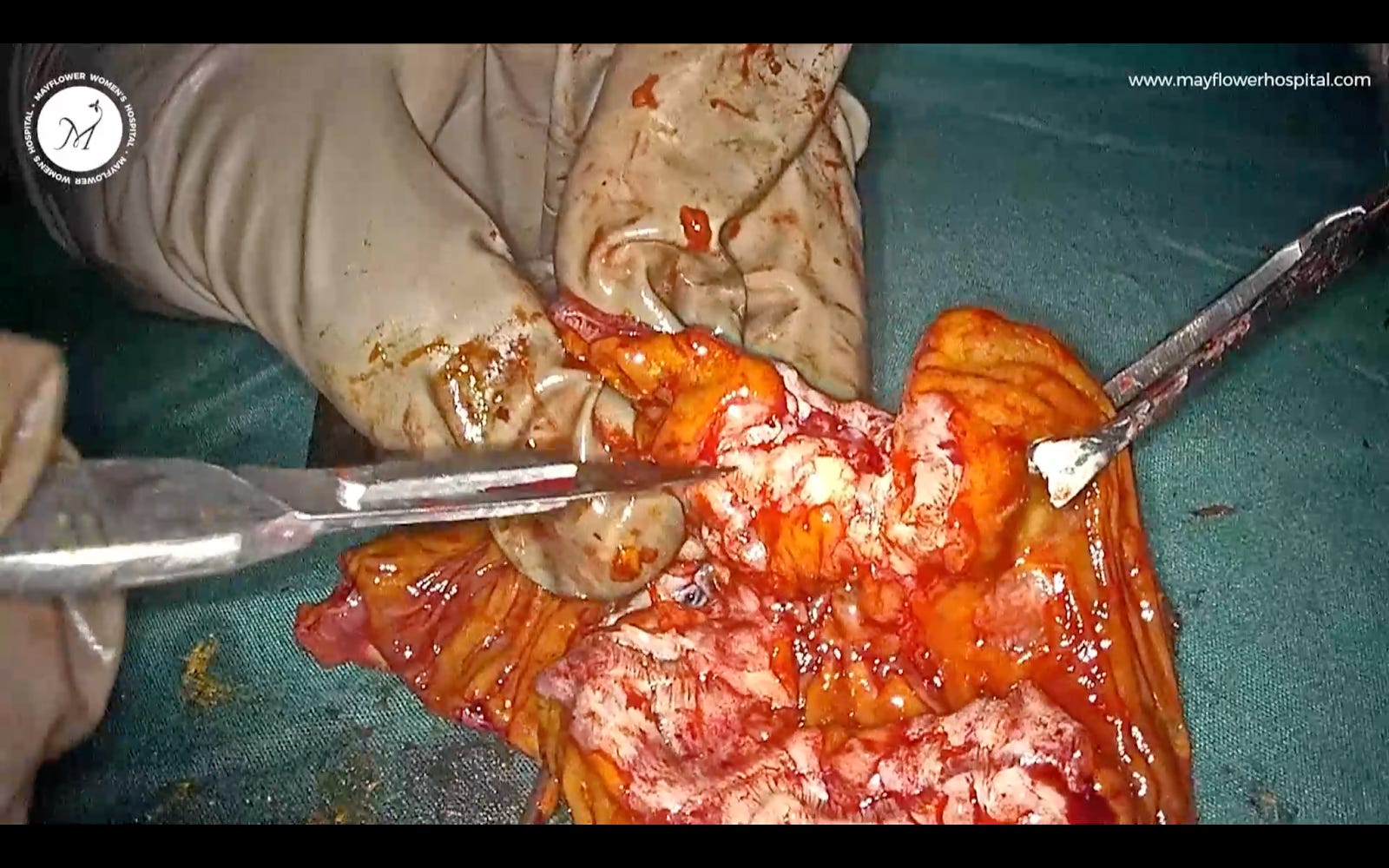
Here you can see the anastomosied specimen. And below is the excised affected part of the small bowel affected by endmetriosis
The colon is now delivered back into the abdomen, and an exit is made.
Here’s the final view before we say tata bye bye and hand it over to the extubation team.
Key Takeaways
Mapping the disease is crucial
Always have a GI surgeon with you
Remember the Rule of M to correctly identify bowel candidates of shaving vs resection and anastomosis
A tension free anastomosis is crucial to a successful surgery
We will soon bring out a detailed video edition of this surgery in a later newsletter. Until then, good luck getting back to the grind post your Diwali break! we hope you have a great week ahead!
 | A guest post by
|
 | A guest post by
|
Get your poop straigĥt and healthy with my podcast here:
https://soberchristiangentlemanpodcast.substack.com/p/s2-ep-13-healthy-bowl-movements-8ef