



Extreme Ureteric Involvement and Re-Implantation
A surgery breakdown of steps involved in handling DIE in the lower 1/3rd of the ureter
It’s No-Sleep-September here at Mayflower. With back to back conferences, training schedules and intensive surgeries, this month has been off to a rather adventurous start. So we thought it’s worth giving you a taste of the same adventure; albeit in endometriosis.
This week’s edition deals with deep infiltrating uretric nodules in the lower 1/3rd of the ureter. It’s probably the most complicated kind of involvement to deal with, not as much becuase of the nature of the disease, but more because of the collateral damage it causes and what needs to be done to fix it.
Also, this edition has been written on an airplane somewhere above the black sea on a Turkish Airlines plane. So please forgive if you happen to see some follies along the way. Here’s a picture before we begin

Alright, back to endometriosis.
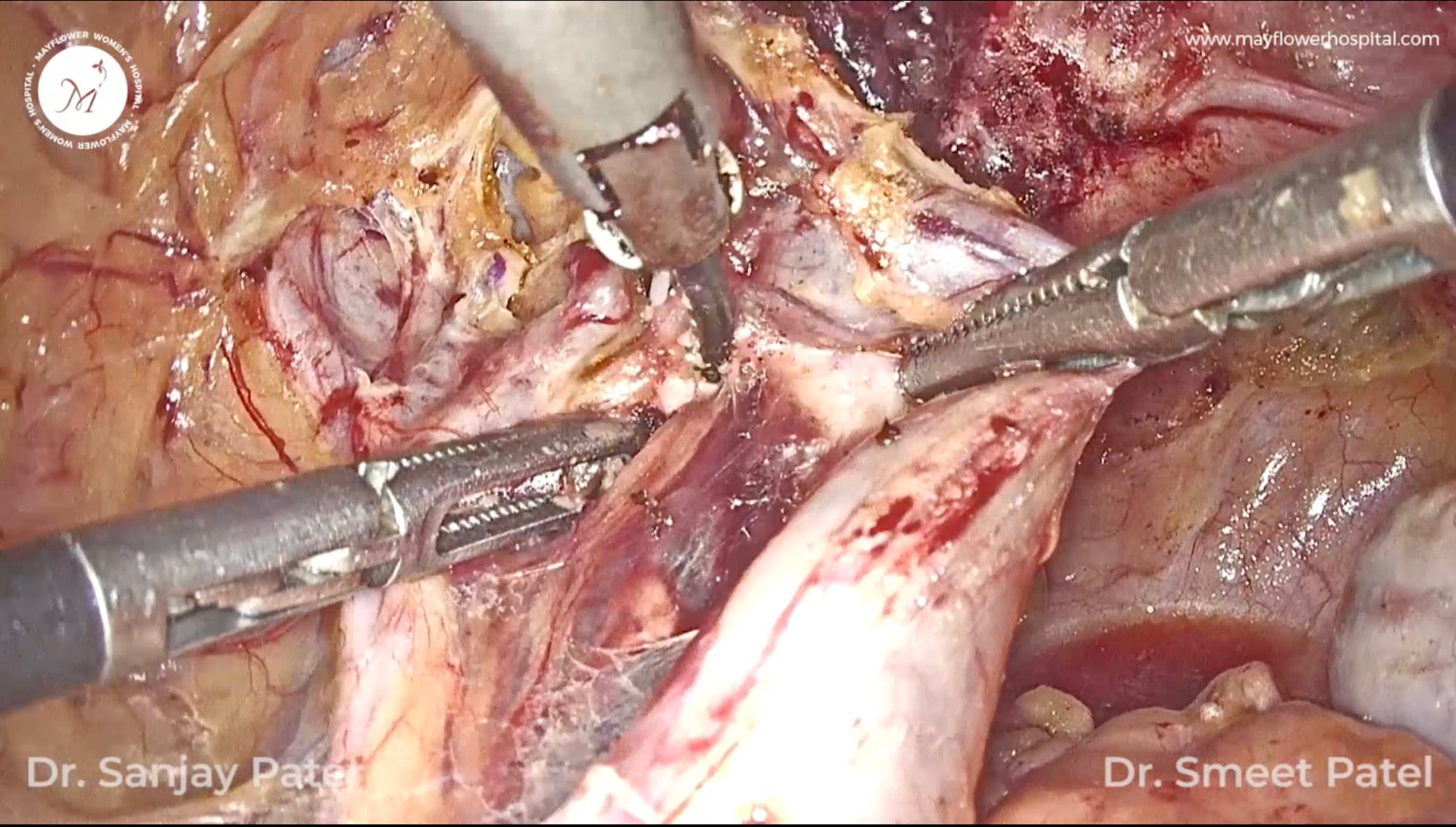
The process begins by disecting the parametrium and all the surrounding tissues. This is something we dealt with in an earlier edition that you can read here
Once cleared, we begin by denuding the ureter. The process of uretric dissection begins from closer to the periphery and moves towards the bladder. The dissection process is slow, fiber by fiber, we tease laterally and cut vertically, and keep moving forward.
The ureter we need to understand, isn’t a typical organ that endometriosis can simply implant on. There are several deterrent that keep the disease away from the ureter.
For one, the ureter is constantly mobile. In surgery, it can be observed to be moving, and this motion makes it a tough target for endometriosis to latch on to.
Secondly, it’s behind a layer of mesentery which itself acts as a barrier for tissue growth.
This means when the disease finally manages to latch on to the ureter and results in symptoms, the involvement will be intense. This is why it is important to first deal with all involvement in various parts of the pelvis before returning to treating the big problem with the ureter.
What big problem? You might ask. There could be two
1. Intrinsic Involvement
2. Sticturing
3. I lied, the third could be both.
Intrinsically involved portions of the ureter must be resected off and a new connection established to restore compromised renal function. For sticturing, it’s a matter of how early or late we catch the disease. Hydroureter, and hydronephrosis must be dealt with completely as they are fatal for the kidney. More on that later.
But before we get there, all endometriotic plaque from the entire genitourinary tract must first be removed. Parallelly, the parametrium will also be dissected and all nodules removed.
Once all is clear, we move to the stictured part. In the case we pick today, the sticturing was found in the lower 1/3rd of the Ureter in the Tunnel of Wertheim.
First all the nodular plaque is removed and a fresh margin of the ureter is taken to be inserted into the bladder.
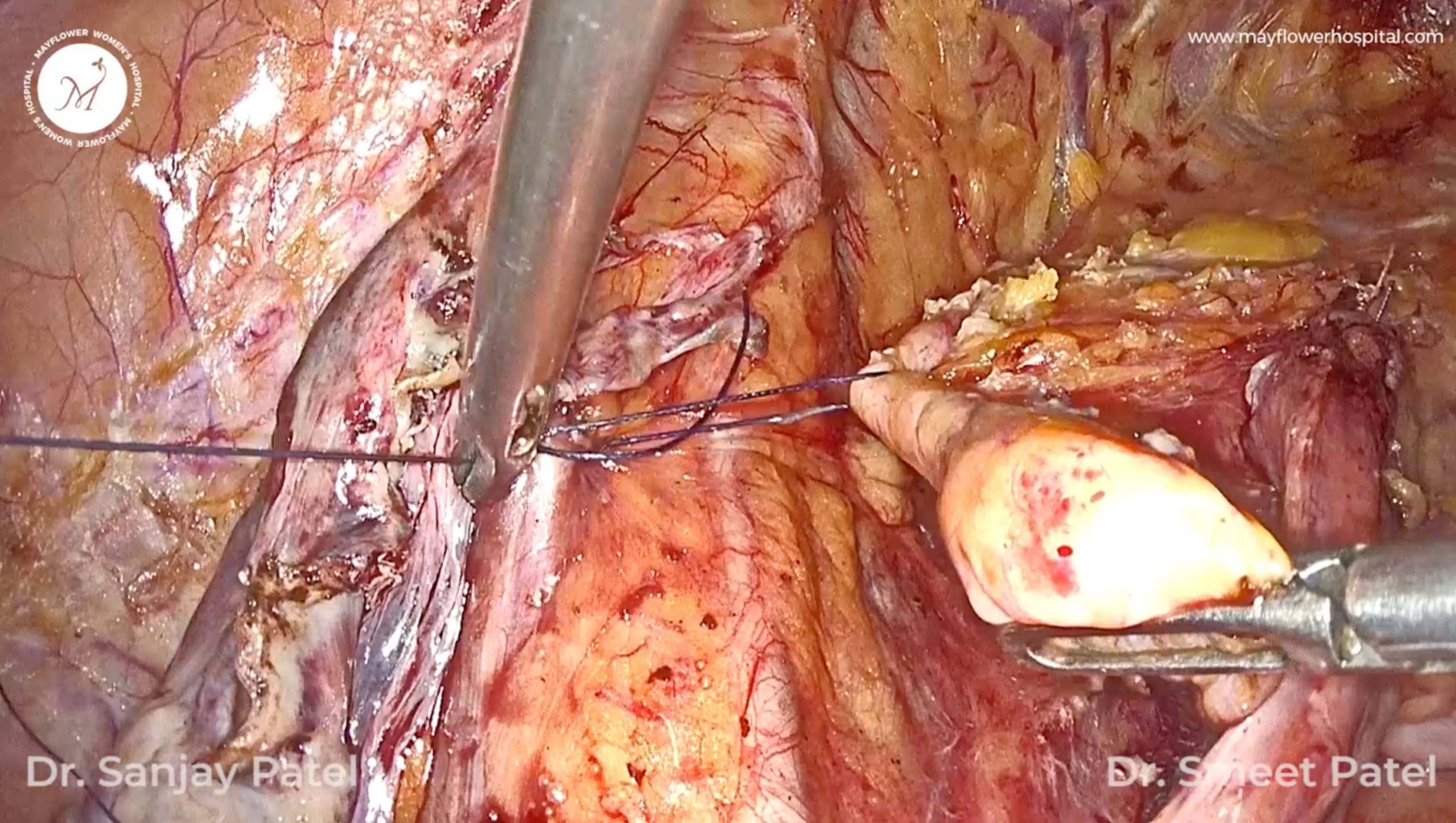
To start the procedure, we pick a point along the healthy proximal margin of the ureter and place a clip to stop the backflow of urine.
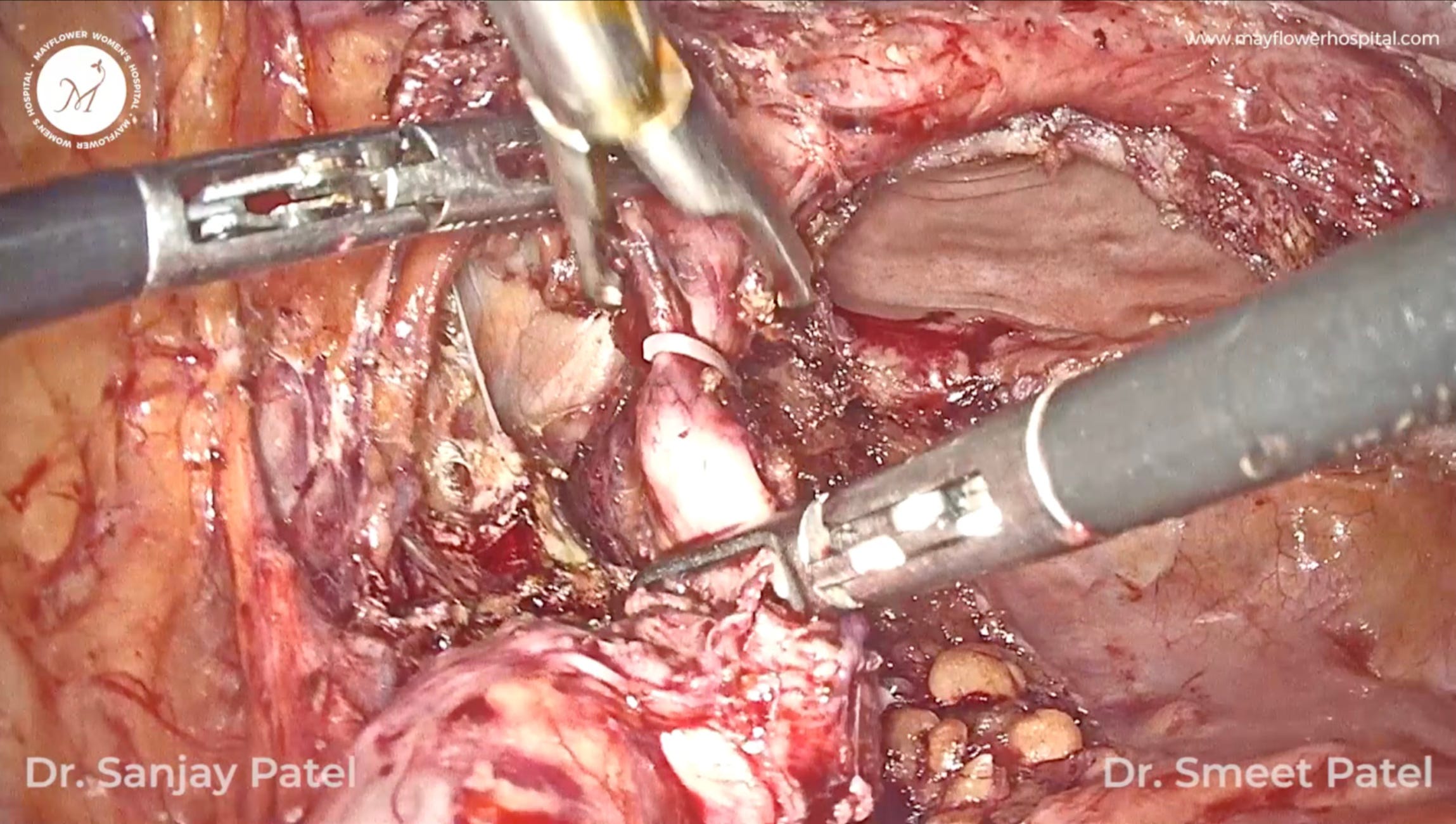
Next, the Space of Retzius is identified and dissected; the ureter is freed of any remaining endometriotic plaque and fresh margins are spatulated.
A small nick is placed in the lateral fundal region of the bladder for implantation. To conduct the implantation, the spatulated fresh margin of the ureter is opposed to the site of implantation on the bladder after which a stitch is taken at 6 o’ clock and a laparoscopic stent is placed.
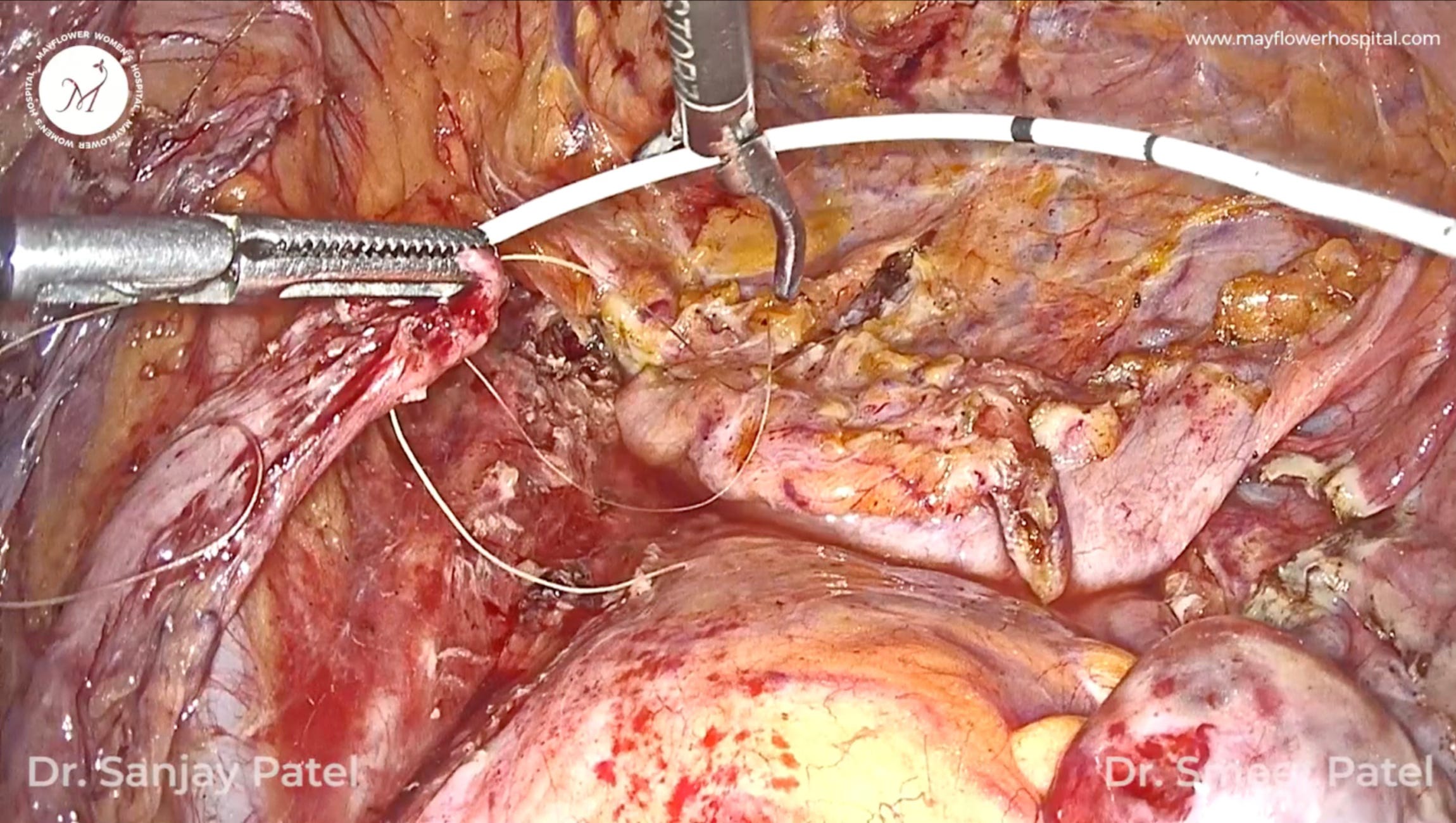
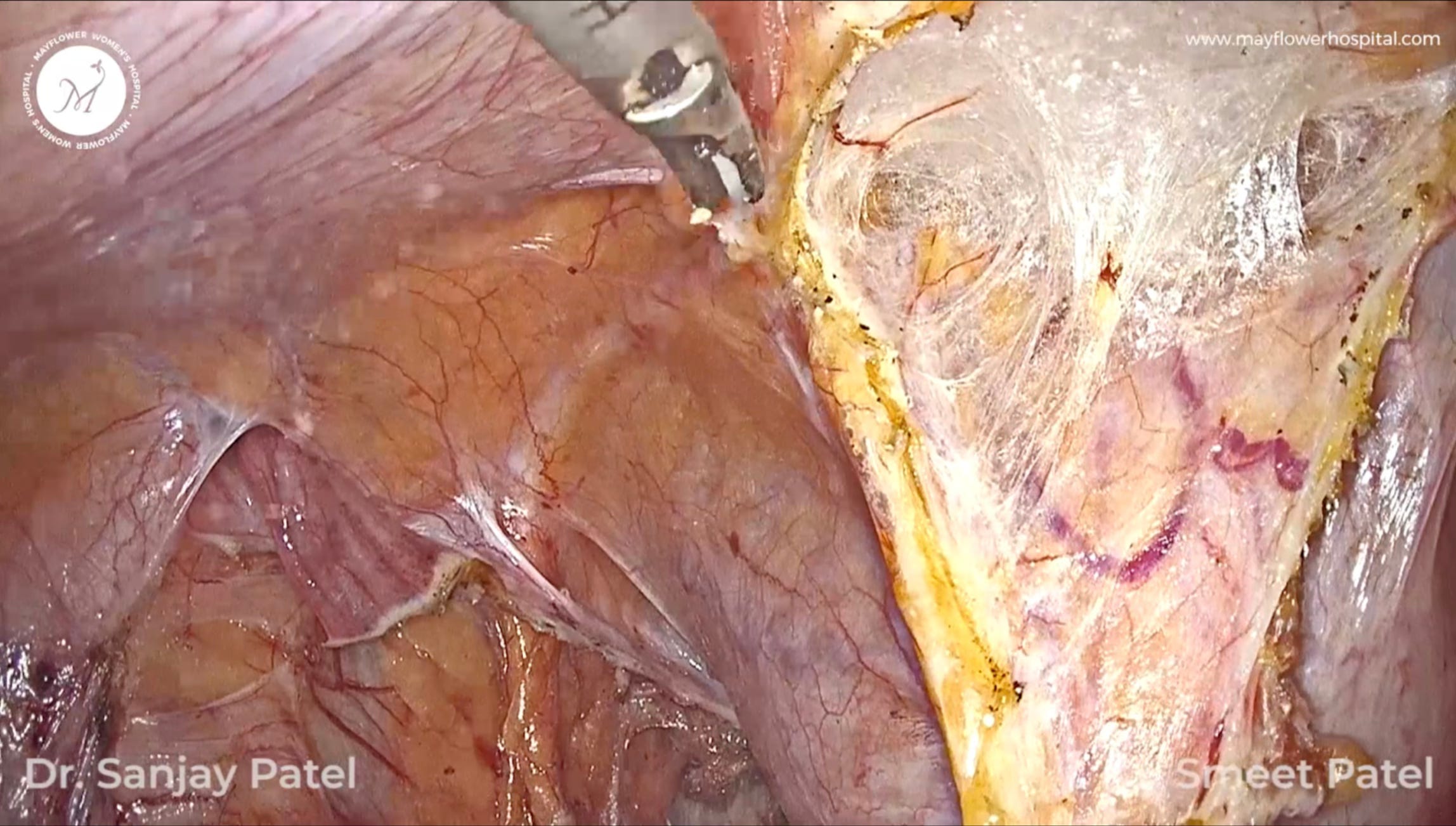
5 more stitches are placed in the periphery to secure the anastomosis along with a psoas hitch to keep the junction tension free. A pseudo tunnel is also made to prevent the backflow of urine.
And finally, this is what the view in the end looks like
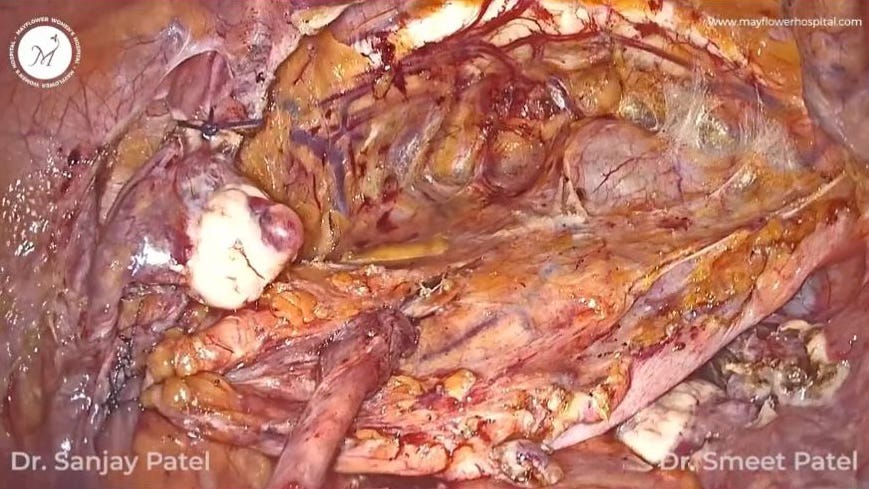
The process is of course rife with all kinds of risks that need to be discussed with the patient beforehand but more importantly, the procedure demands from the entire surgical team a certain level of patience, rigour, and mitculouslness that will remind you of school again.
That’s it from us this week. We’ll see you next week with more endometriosis and some picture from Prague and Vienna.
See you!