



Trishla's encounter with parametrial Endometriosis
Delayed surgeries in endometriosis are the most harmful tendancies that patients present and often, doctors empower.


Following is a true story. At the request of the patient, their name has been changed. Out of respect for the practice of surgery, the rest has been told exactly how it occurred.
Trishla Pandey, 26, visited Mayflower on the 4th of October 2022 with a complaint of persistent abdominal pain. Chronic. She could barely wait in the lounge. With cases of deep infiltrating endometriosis, this isn’t too uncommon. But very soon, we were all going to find out that Trishla’s condition was.
Hailing from a family of businessmen based out of North India, Trishla has been seeing her gynaecologist for a long time with the complaint of painful periods. Over the years, this complaint had developed into chronic pain. Two times during her consultations with senior gynaecologists, she had been referred to surgery, “I really want to avoid it as much as possible” she would tell every doctor that her family took her to.
No one loves going under the knife. Surgery avoidance is a major issue that aggravates several conditions across a broad spectrum. Endometriosis however, because of its taboo, and the wilful ignorance of people, doctors and patients alike, suffers on the far end of that curve.
On an average, a symptomatic woman will go 6 to 7 years before she gets diagnosed with endometriosis. A decision for surgery then taking even longer. In Trishla’s case, this period was 9 years. “I just want the pain to stop. That’s all. I don’t care if I can have kids or not. Just help me live life again…” she said as we sat in the consulting room discussing what she wanted out of the treatment.
Parasar, Ozcan, & Terry, Endometriosis: Epidemiology, Diagnosis and Clinical Management, 2017
That only seems fair. Her life had come to a standstill. Outings with friends and family had to be short, trips were limited, and she always had to have pain meds on speed dial. On good days it was difficult, on bad days, morbid.
Given the history itself, we knew that she was going to need special care and attention. An MRI was ordered and our suspicions solidified what sonography suggested.
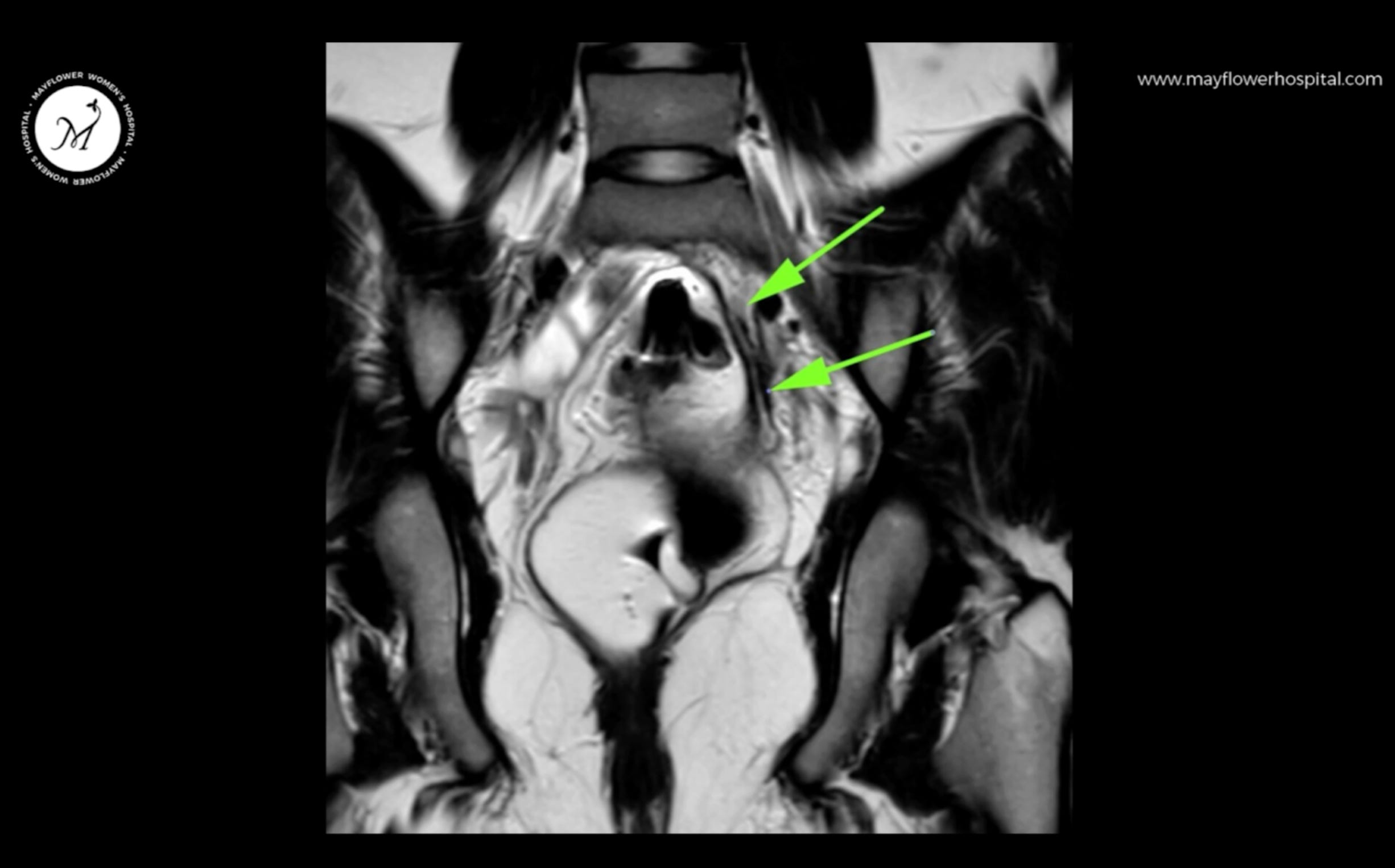

The parametrium is new for this audience. We haven’t talked about it before, you and I. It is a region formed by the round ligament, the broad ligament, the cardinal ligament, and the uterosacral ligament along with the area beneath the peritoneal fold and inclusive of the pelvic lymph nodes.
Often involving the S3 S4 S5 segments of the sacrum, parametrial involvement is a major cause of chronic pelvic pain, not just cyclical discomfort or morbidity. This leaves an irreversible trauma on the minds of people who suffer through this disease. In large parts, the agony of women who suffer a terrible fate at the hands of this disease, goes unnoticed.
Treating involvement of the parametrium is a difficult job, even for the more seasoned surgeon, which is why preparedness is critical in cases like these.

Along with showing signs of parametrial involvement of endometriosis, Trishla also had a rare congenital anomaly of a Robert’s uterus, it was discussed that that’s also something we would try and rectify in the process of surgery.
Upon entering, we can clearly visualise the disease involvement on the left side.
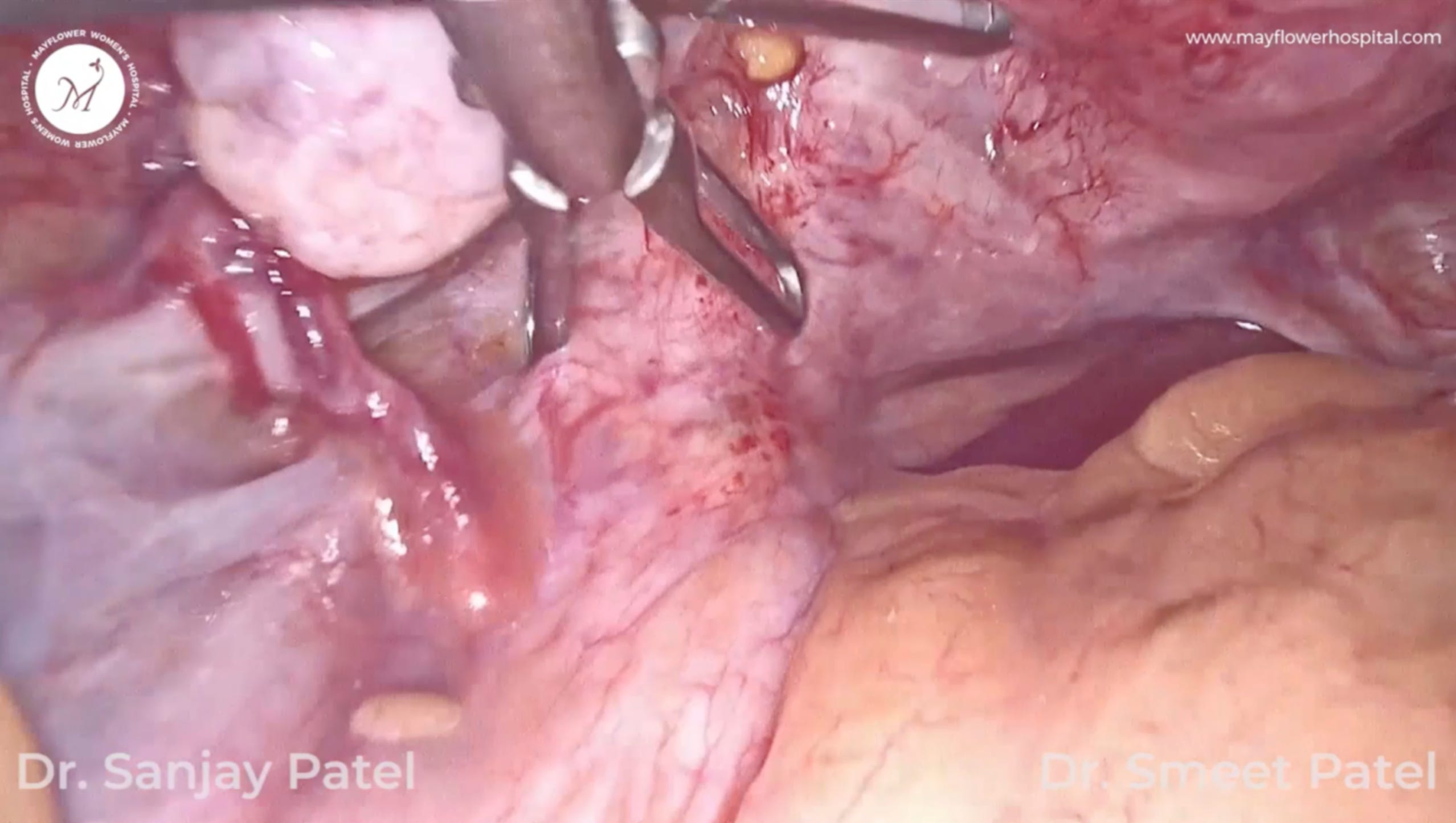
The lateral pelvic vessels like the internal illiac artery and vein are major landmarks that need to be protected in the process of carrying out this dissection. Which is why it is important that we stay in line with the fundamentals of operating in altered anatomies.
Here’s a quick refresher:
Proper traction and counter traction
Energy devices always fired carefully, and in short bursts
Dissect fibre by fibre. Slowly but surely.
Predictive anatomy - when dealing with distorted anatomies
There are more, but for now, we get back to the surgery.
Dense adhesions and endometriosis plaques from the pelvic brim all the way to the tunnel of Wertheim is what cause Trishla the continuous and excruciating pain that she complained of.
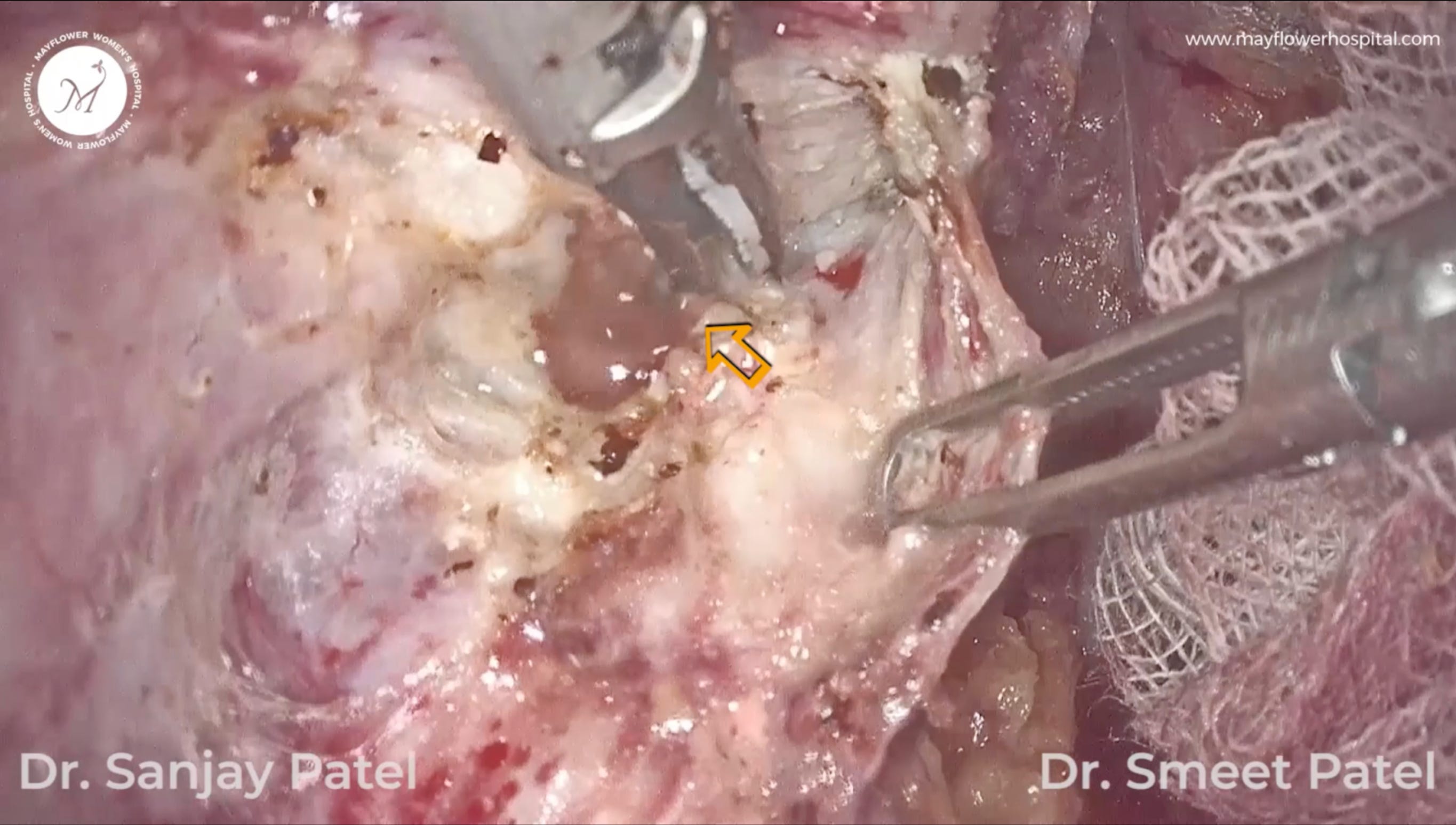
In the course of this procedures, nodules over the ureter - medial to its structure are dissected off along with the nodules over the torus uterinus before we bisect the broad ligament. Next, we take the nodules over the tunnel of Wetheim.

Here is this image where you can see the long and deep red segment of the dissected part of the ureter. The ultrasonic scalpel is currently dissecting a nodule off from a region medial and anterior to the internal iliac vein. Right below this dissection lies the sacral plexus.

It took us nearly 3 hours, 3 surgeons, and a lot of patience, and love, to deal with this case. Trishla visited us just last week, almost 18 months post surgery and we’re happy to report that she found exactly the life that she was looking for. Peaceful, pain free, and liberated. A Trishla who once trembled and shook at the name of surgery today is a champion for the surgical method of treating endometriosis.
The knife gives everyone anxiety. But in the hands of the right surgeon, a knife gives life, and the promise of prosperity.
That’s all for today’s edition. We hope it helped you look at the symptomatic aspect of specific disease involvement more clearly.
Feel free to question and critique anything you don’t agree with in the comments below.
Until next time!
 | A guest post by
|
 | A guest post by
|
This is like a guide for an endo warrior 👏