



A Long Way From Home: Thoracic Involvement of Endometriosis


Good evening friend,
Last week has been spent really contemplating this one surgery that we performed at Mayflower. The kind that only comes once in a long time, and even then demands that we be just as prepared for it. Today’s edition is about an extra pelvic involvement of endometriosis. All the way up on the diaphragm.
Particularly bothersome, particularly tricky.
We thought endometriosis was complex enough when it was invading into every single organ system inside the pelvis. Sure we’ve heard that it often even invades into the brain but you never expect to encounter it. Until you do.
While endometriosis most commonly involves the pelvis, particularly the ovaries, cul-de-sac, broad ligaments, and uterosacral ligaments; endometrial tissue can be found outside the pelvis in various locations including the abdomen, thorax, brain, and skin.
Of these, thoracic involvement is the most frequent extra-pelvic location of endometriosis

Thoracic endometriosis should for the most part be suspected in young females with catamenial pneumothorax or hemothorax during their reproductive age. The likelihood is especially high in those who have a history of prior uterine surgical procedures or proven pelvic endometriosis (present in 56 to 84 percent).
The most common site? The right hemidiaphragm — likely due to clockwise peritoneal fluid circulation and liver barrier effects that spare the left side.
This pathology typically presents with:
Catamenial pneumothorax (the most common, up to 80% of cases)
Catamenial hemothorax
Catamenial hemoptysis
Pulmonary nodules or chest pain synchronized with the menstrual cycle
The timeline is diagnostic: symptoms appear 24–72 hours before or after menstruation, rarely up to 96 hours. Pain is typically right-sided, often scapular or subcostal, and may be confused for musculoskeletal or gastrointestinal issues in early stages.
Why It Happens: Theories of Long Distance Spread
The pathogenesis remains multifactorial, with several theories at play:
Transdiaphragmatic passage: Endometrial tissue migrates through congenital or acquired fenestrations in the diaphragm.
Microembolization: Endometrial cells enter the venous or lymphatic system and travel hematogenously to the lungs.
Coelomic metaplasia: Thoracic mesothelial cells differentiate into endometrial-like tissue under hormonal influence.
Direct extension: Diaphragmatic lesions may penetrate upwards into the thorax over time.
Thoracic endometriosis is not rare, just rarely diagnosed.
In women with pelvic endometriosis, studies suggest up to 56–84% may have thoracic involvement when evaluated thoroughly.
Management
Like all complex surgeries (or tasks in life) it’s the team that makes it happen. The management of patients with this problem frequently involves multiple disciplines including pulmonologists, thoracic surgeons, good anaesthesiologists and gynaecologists.
It’s a true multidisciplinary affair — because operating near the lungs, diaphragm, heart, and vessels? Not exactly a solo mission.
The gold standard?
Surgical excision. And here’s where it gets even more fascinating
A Peek into the Procedure
Mapping the Disease
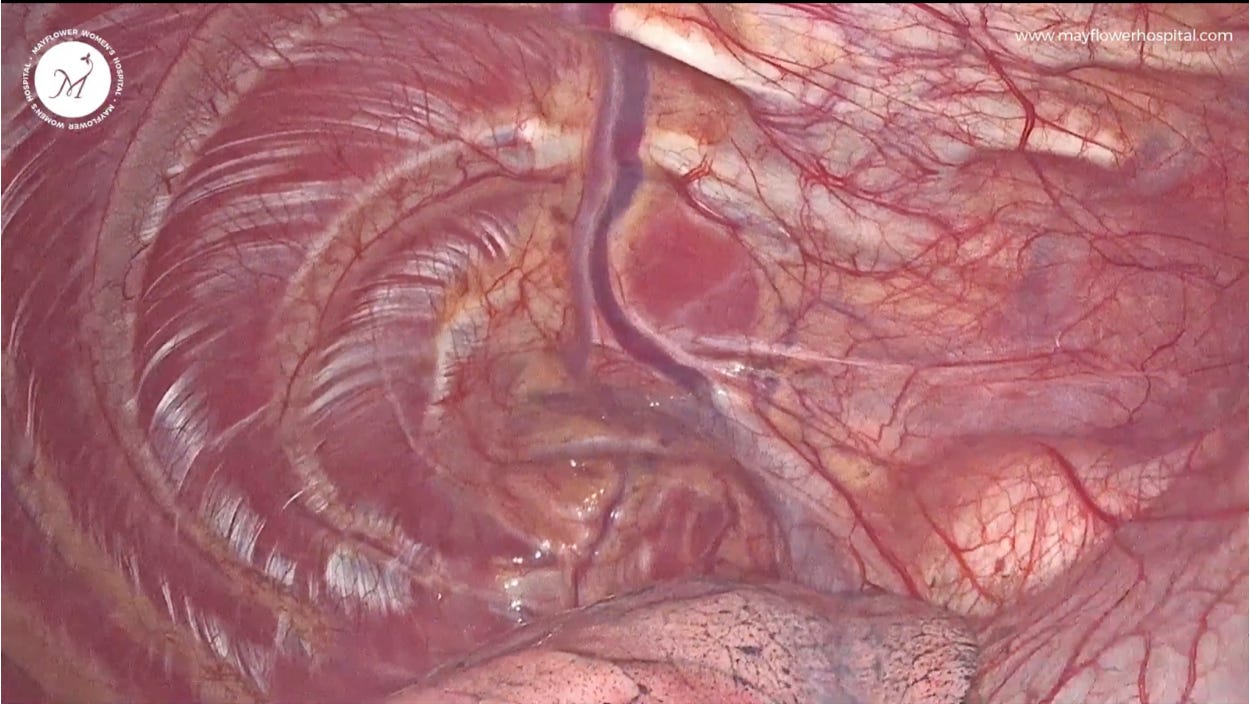
The first step is accurate mapping — visualising both the pelvic and diaphragmatic disease. Lesions on the diaphragm may be superficial (amenable to shaving) or deeply infiltrative, requiring segmental resection.
Shaving works when nodules are peritoneal-based — similar to how we approach the rectovaginal septum. But if the lesion has breached the muscle layer or shows fibrosis tethered to thoracic structures, full-thickness excision of the diaphragm is required.


Crossing the Border: Entering the Thoracic Cavity
When we open the diaphragm, we truly move into a multi-specialty territory:
You may visualise the lung parenchyma, azygos vein, phrenic nerve, internal thoracic vessels, and even cardiac pulsations.
The anaesthesiologist (in our case Dr. Sanjiv Upadhyay) becomes central to the procedure — managing positive pressure ventilation to prevent pulmonary collapse as abdominal CO₂ insufflation threatens to enter the thoracic cavity.
Conclusion: A lung-protective strategy must be in place; otherwise, you risk significant respiratory compromise.
The Technique: From Excision to Closure
After a complete excision of the disease we first close the diaphragmatic defect using V-Loc sutures in a non-locking continuous pattern.
Our goal is to establish a tension-free, airtight seal — especially important to prevent postoperative pneumothorax or paradoxical diaphragmatic motion.
Here’s the nuance:
At the final closure, we introduce a suction cannula into the thoracic cavity to evacuate residual air, then simultaneously pull the cannula while completing the last stitch. This technique creates a vacuum closure, eliminating the need for a thoracic intercostal drain (ICD) in most cases.

It’s elegant, efficient, and reduces postoperative morbidity.
Why This Matters
Too many women live with undiagnosed thoracic endometriosis — repeatedly misdiagnosed with asthma, musculoskeletal pain, or spontaneous pneumothorax with no apparent cause.
Early recognition requires clinicians to think beyond the pelvis.
And managing it? That takes a collaborative OR, anatomical precision, and a refusal to let endometriosis keep rewriting the rules unchallenged.
In Conclusion
Thoracic endometriosis is a stark and likely frequent reminder that this disease is not confined to the reproductive tract — it’s a systemic disorder capable of migrating, infiltrating, and mimicking a wide array of conditions across multiple organ systems.
While surgical excision of diaphragmatic and pleural lesions offers effective relief and is often curative when done comprehensively, it is not without its challenges — or its consequences. Postoperative adhesions, recurrence, and the potential for persistent neuropathic pain at the chest wall or shoulder can complicate recovery.
In rare cases, thoracic endometriosis may extend into the lung parenchyma itself, leading to chronic pulmonary changes or repeated catamenial hemoptysis.
Even more rarely, central nervous system involvement has been reported, and cerebral endometriosis — though exceedingly uncommon — underscores how systemic this disease can become when unchecked.
There’s also the fertility conundrum: patients undergoing major excision for thoracic disease often have advanced pelvic endometriosis as well, and reproductive planning must be integrated into their long-term care strategy next to giving them a healthy and normal life. Both can go hand in hand, if we try.
Ultimately, thoracic endometriosis requires us to move beyond a “gynecology-only” lens. It demands multidisciplinary surgical coordination, high suspicion, and personalized planning that addresses the full spectrum of disease — from pelvic to pleural.
Because when endometriosis breaks out of the pelvis, we don’t just follow it.
We meet it there — and we cut it out.
 | A guest post by
|
 | A guest post by
|