



The Unofficial Symptom Map of Endometriosis
Correlating symptoms with disease occurrence in Endometriosis is hard but latest research provides some relief


The moment someone finds out about Endometriosis and why it is caused, the next question they have is, “How do I know I have it?” And funnily enough, the scientific answer to this question is an emoji. This is the emoji: 🤷🏻
But patients don’t understand this. They need answers. So today, we’ve put together the Unofficial Symptom Map of Endometriosis. Collated from various publications, and surgical findings, this map is a broad spectrum understanding of the sensation the disease might give to an incumbent patient and some correlating surgical images and findings.
Is this map exhaustive? No. Which means there could be symptoms and involvements it does not consider. Is this map exclusive? No. This means there could be symptoms that are triggered by more than one type of involvement.
Is this map helpful? Definitely.
We will go symptom by symptom and try to see what involvement and intensity they may relate to and where we could find them on a diagnostic stage if possible.
Asymptomatic
Asymptomatic patients are the most difficult cohorts to have a conversation with in any field of medicine. Breaking a news to someone who is least expecting it, is a tough job, and every day is an attempt at becoming better at doing so. We often see infertility as a symptom which is more removed from the other symptoms which are typically painful.
Dyspareunia
Or pain during sex is a fairly common complaint in cases of endometriosis. With deep infiltrating endometriosis, this complaint is more stark, the symptom more apparent and hindering. Most complaints of dyspareunia can be correlated with caudal occurrence of endometriosis on the recto-vaginal facia. Deep infiltrating implants may even cause parallel gastrointestinal symptoms like dyschezia.
Proximal (Deep) Dyspareunia is caused mainly by endometriosis tissue growth in the periphery of the posterior aspect of the vagina. This pain gets triggered when the patient indulges in deep penetrating intercourse, or other penetrative activities. Nodules along the uterosacral and cardinal ligaments, Pouch of Douglas (cul-de-sac), posterior vaginal fornix, and anterior rectal wall are often key conspirators for the symptom.
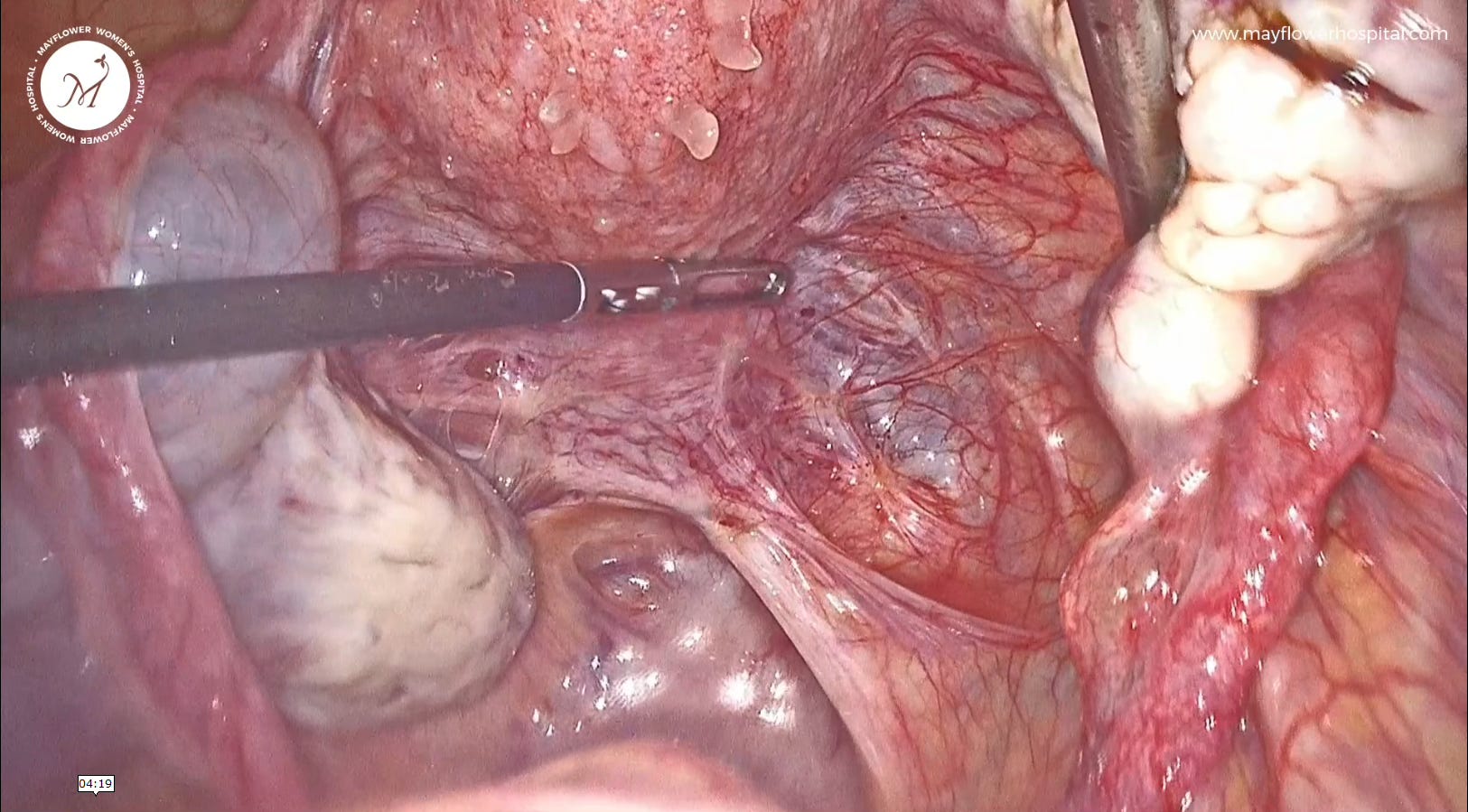
Distal (superficial) dyspareunia, also called superficial dyspareunia, is known to often result from lesions of the cervix, hymen, perineum, and sometimes from episiotomy scars. Development of the disease specifically around tissue recovery from trauma (like scars) has been of special interest to us over the last several years.
Post op adhesions, and growth are fairly common and in our experience a result of incomplete or no disease removal at the time of a previous procedure.
Urinary frequency, Urgency, and/or Painful Micturition
Bladder endometriosis typically presents with nonspecific urinary symptoms of frequency, urgency, and pain at micturition. This symptom set can worsen with menses. However, ureteral endometriosis can be asymptomatic or at best associated with colicky flank pain or gross hematuria. This makes ureter a silent victim of endometriosis and it’s often very late by the time people find out about it.


What adds to the problem is that a person suffering from endometriosis may or may not see a gynecologist when their symptoms are renal troubles. There’s that old radiology dictum, “if you’re not looking for it, you might miss it” And that often happens in cases where endometriosis is not in the specialist’s consideration at all.
Fortunately, as the years go by, more and more specialities, specifically gastroenterology and urology are becoming more aware of the presence of this disease that as
Diarrhoea, constipation, and/or abdominal cramping
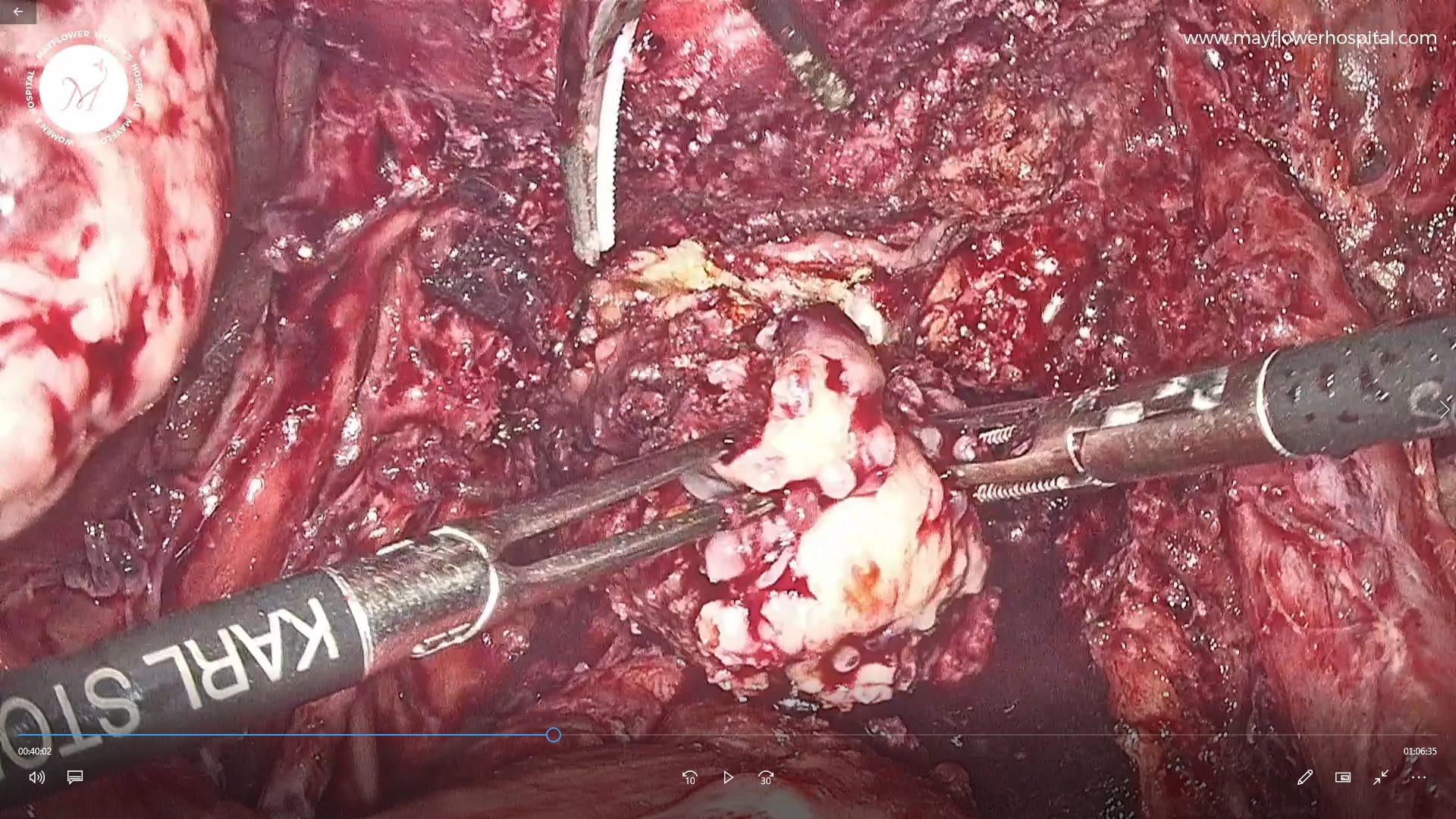
Bowel endometriosis is a tough nut to crack. We often rely solely on MRIs for surgical planning as the degree of cross sectional and circumferential involvement of the disease over the large intestine is key in determining how the treatment happens.
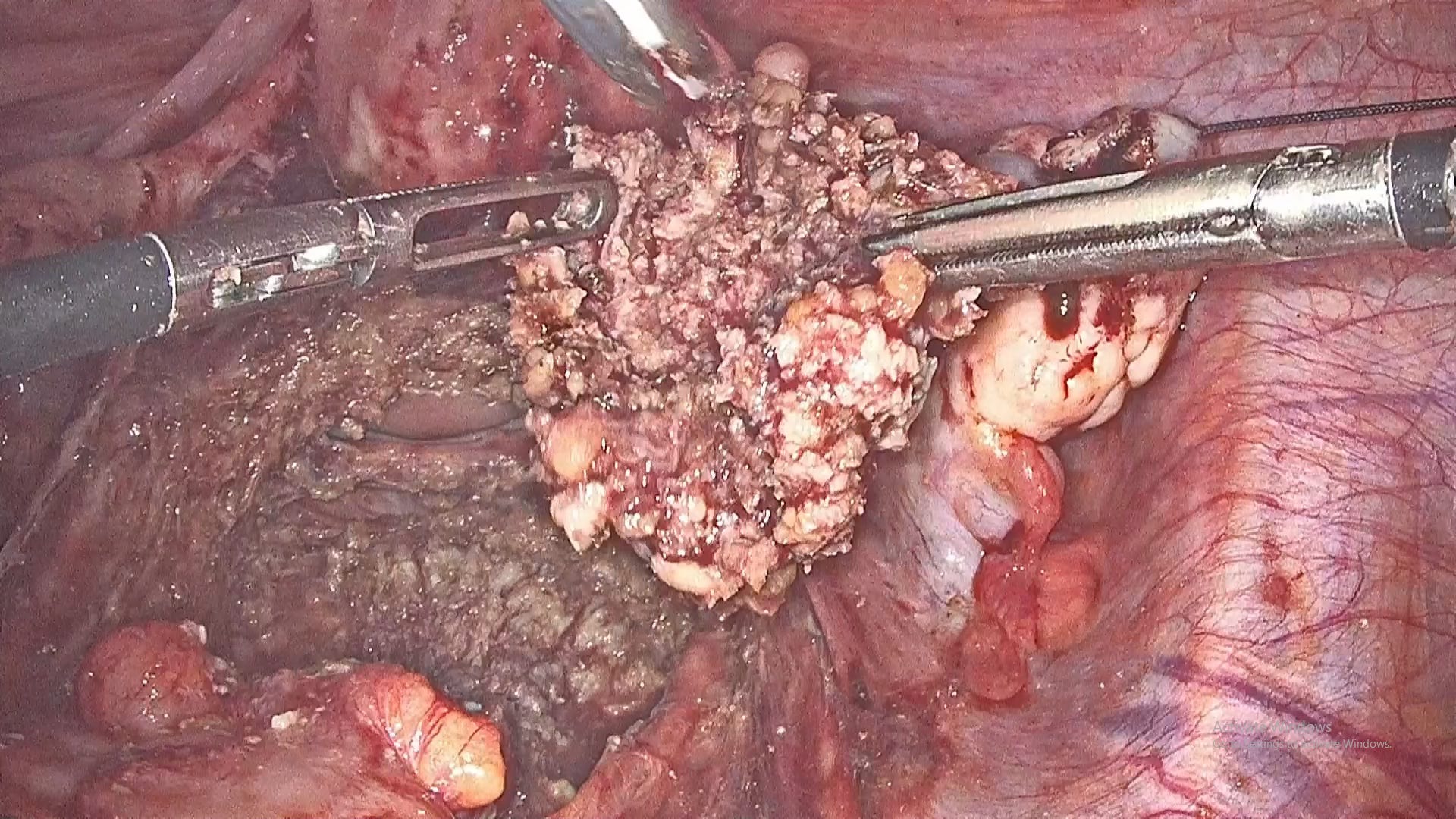
The most common set of symptoms involves diarrhoea, constipation, dyschezia (pain while passing stool), and bowel cramping. DIE implants on the posterior cul-de-sac (PoD) and rectovaginal septum typically present painful defecation along with dyspareunia. Rectal bleeding may occur but is rare.
Abdominal wall pain
Often directly associated with endometriosis of the abdominal wall, pain in such cases is cyclic with menses. However if the disease is long harbored, the pain may even become chronic and difficult to control. In some cases, interestingly, cyclic bleeding has also been reported with vulvar endometriosis.
And there you have it, the very basic hitchhiker's guide to endometriosis. A map of the disease and where the clues of symptoms can take us. We’ll see you around next week!
 | A guest post by
|
 | A guest post by
|
Nice explanation