

The Sanjay Patel Classification of Adenomyosis
A simple and effective 5 grade classification developed by Dr. Sanjay Patel for categorising and treating Adenomyosis


Adenomyosis, or endometriosis interna is a tricky condition. While its occurrence significantly increases the likelihood of endometriosis externa, it is also a contributor to some of the most commonly known symptoms of endometriosis.
Heavy and prolonged menstrual bleeding, severe cramping or sharp knife-like pelvic pain during menstruation (dysmenorrhea), chronic pelvic pain, and painful intercourse (dyspareunia).
In addition, adenomyosis also contributes significantly to infertility, which is often a chief complaint patients approach you with.
Beginning in the mid-90s up to 2010, Dr. Sanjay Patel’s challenges in treating patients with adenomyosis were plenty. To begin with, it was a challenge to measure how intense the disease was.
To add to that, the concurrence of single focal tissue growth along with diffused disease typical of adenomyosis, couldn’t be characterised by a single number of the size of a focal growth.
Internally, doctors used to (and still do) refer to a uterus by the relative size of a pregnant uterus in weeks. This again was just a proxy for size and therefore only informed the listener of half the disease.
But most importantly there was the problem of procedure standardization. The understanding of a disease and its quick classification aids surgeons in deciding the procedures they need to undertake to fix the disease.
These issues presented a pressing need for a classification for adenomyosis. One that would account for the size of growth as well as the presence of diffused disease within the rest of the myometrium.
Today, we take a look at the Sanjay Patel Classification of Adenomyosis and how it can aid in understanding disease incidence better.
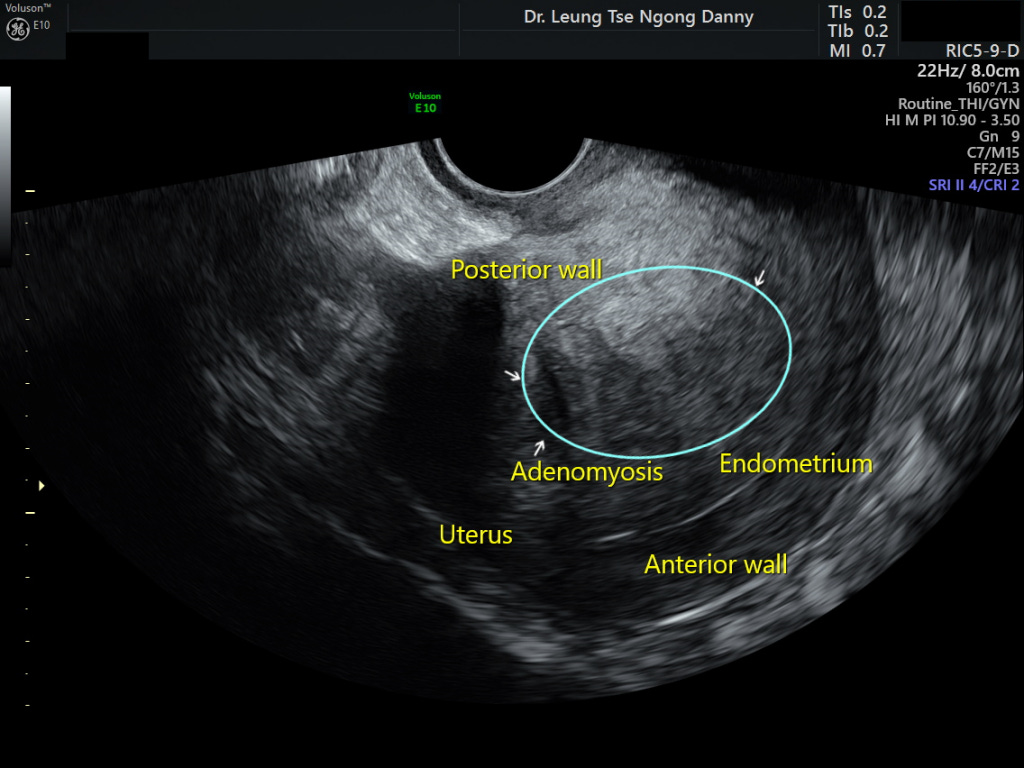
The first point of diagnosis is a trans-vaginal ultrasonography and you can typically expect to see a posterior thickening of the myometrium along with instances of myometrial cysts, linear striations radiating out from the endometrium, and a general loss of a clearly defined endometrial border coupled with an increased myometrial heterogeneity.
With an ectopic growth of endometrium-type tissue, we also see an increased vascularity in the region, observed through a Colour Doppler view. This vascularity also to a great extent helps us define the inner margins of the adenoma.
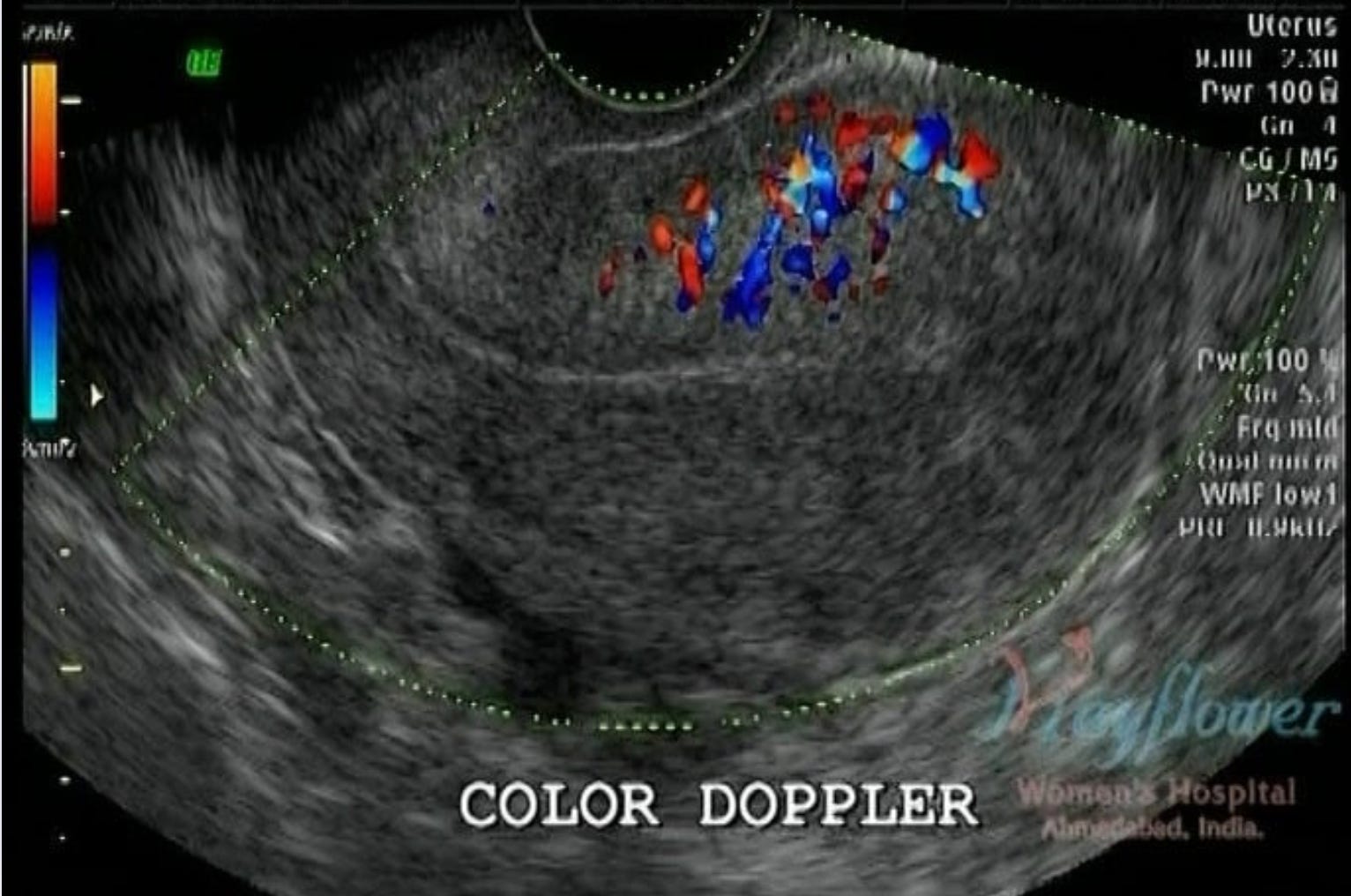
You can appreciate the core of the diseased region in the image above. Because of a lack of a clear margin of the disease in adenomyosis, this vascularity is a good approximation of that margin. In a different edition, we will talk about how this information aids surgical planning.
An MRI can further aid our decision-making. With the aid of the right radiologist, you might even discover previously unknown occurrences of the disease in other parts of the pelvis

For adenomyosis, we want to look for
Any large focal mass
Cystic occurrences
Striations
Put together, these will help us classify the disease into the following grades.
Grade IA
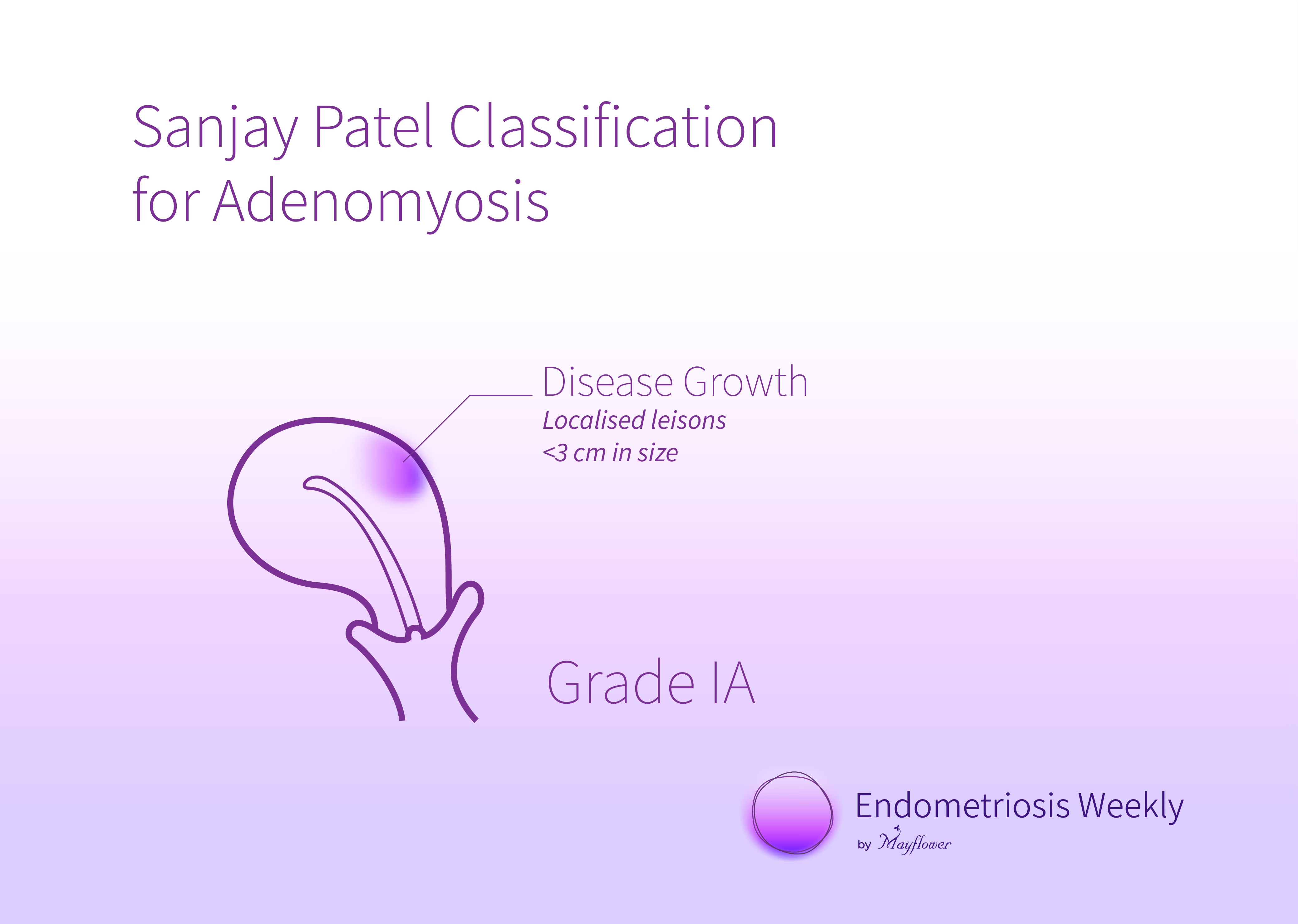
Characterised by localised lesions up to 3cm in size, this is the most basic, low-intensity version of the disease.
Grade IB
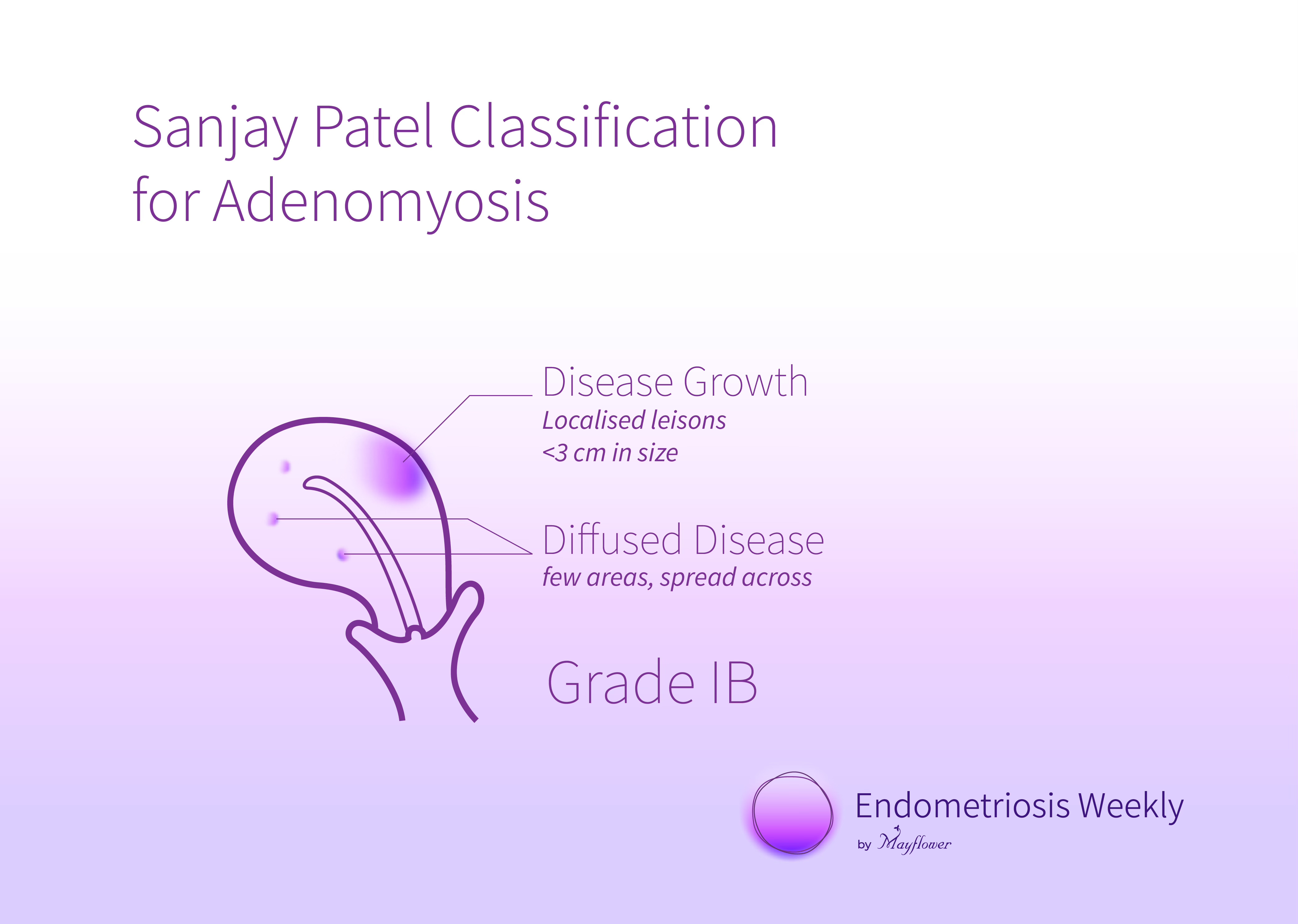
Found alongside diffused instances of the disease across the uterus (both posterior and anterior) this grade indicated a slightly more spread out occurrence of the disease.
Grade IIA
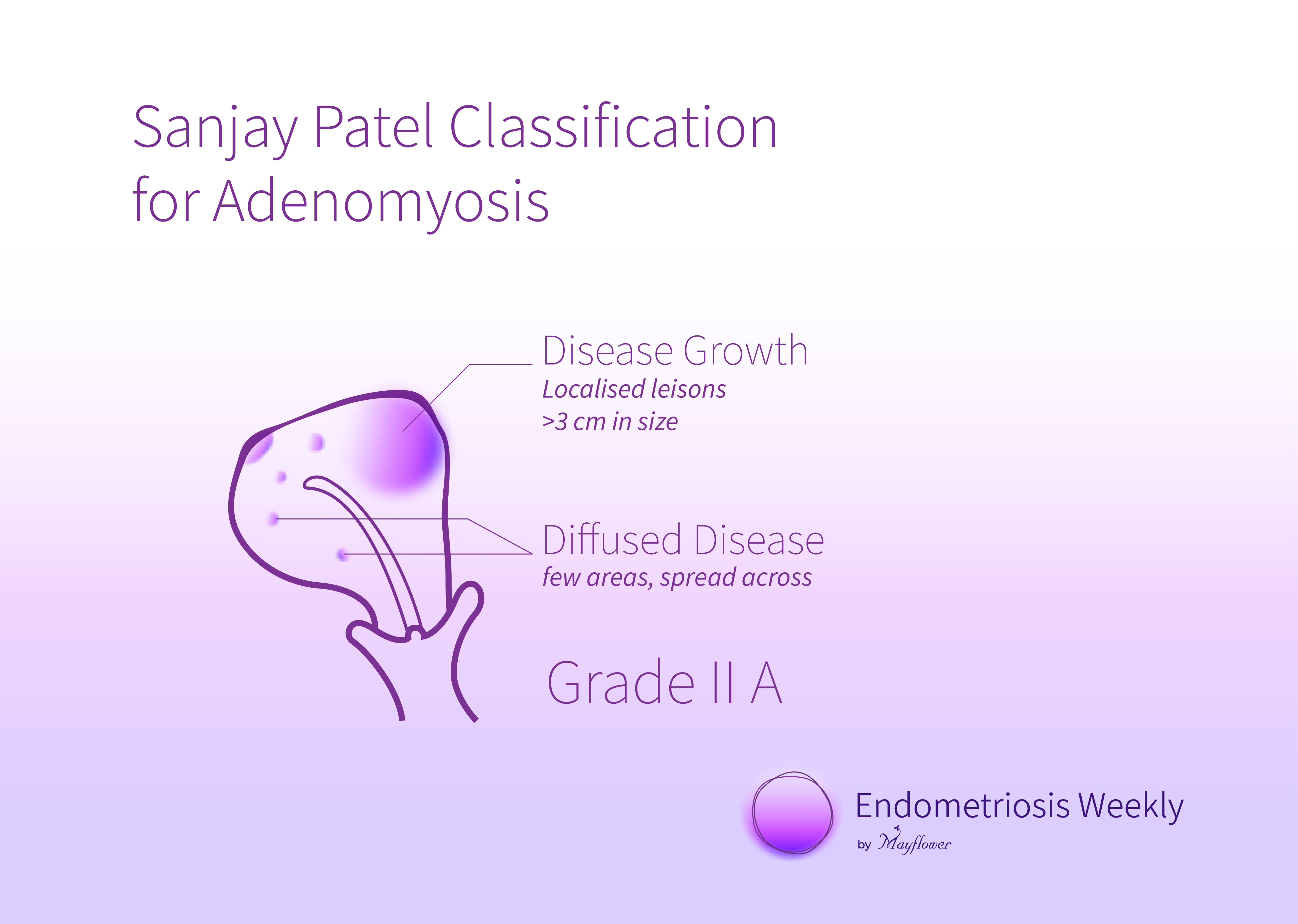
Grade 2A is typically characterised by larger focal mass growth, more than 3cm in size and is often seen alongside a greater occurrence of diffused disease or even a smaller focal growth in a different part of the uterus.
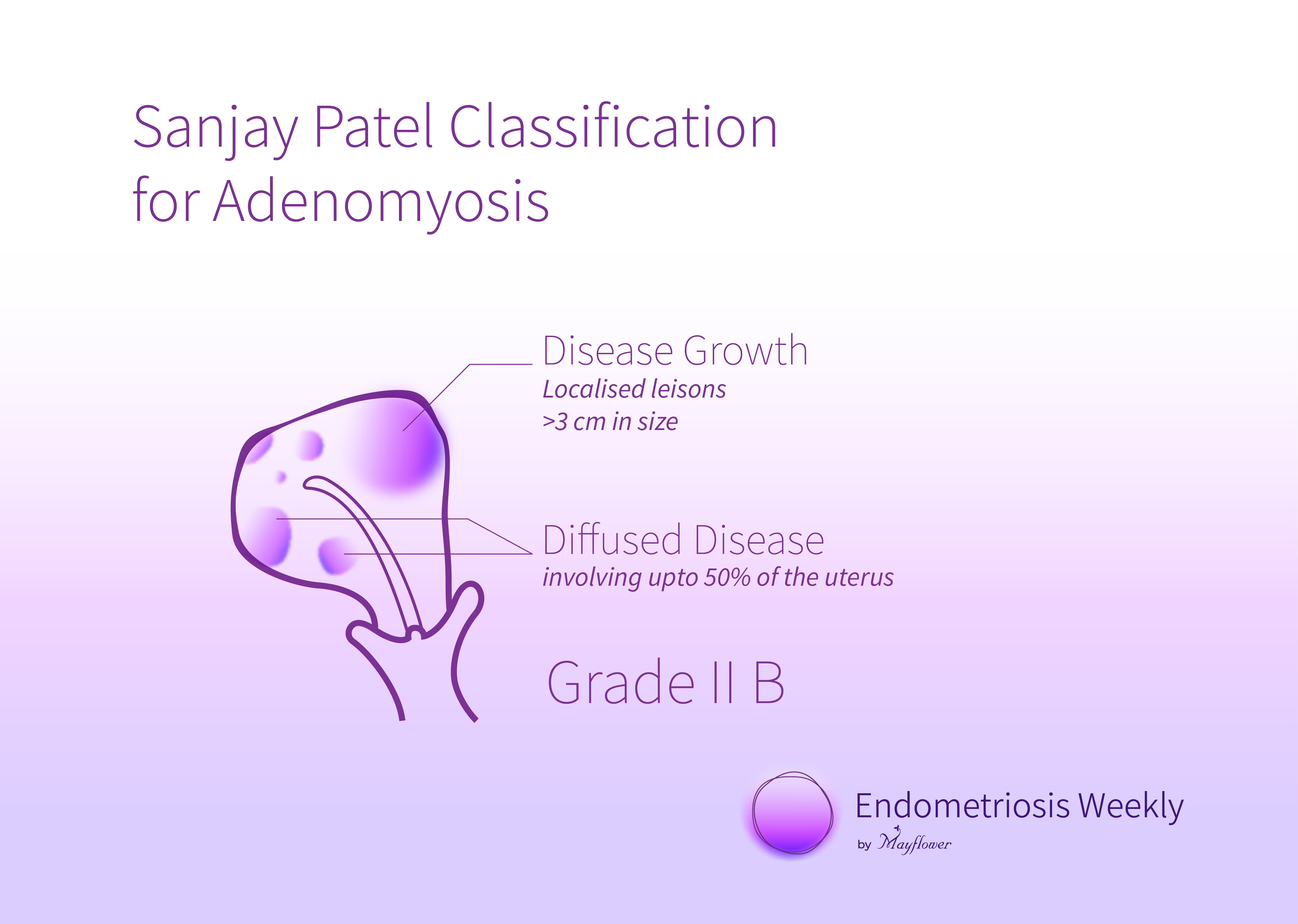
Grade IIB
Moving along the axis of diffuse disease intensity, a Grade 2B adenomyotic uterus is characterised by diffused disease taking over up to 50% of the uterus volume in total.
Measuring the extent to which diffused disease invades the uterus is critical as it defines your surgical path going forward. At this juncture, sharpening your sonography skills to detect patterns of disease occurrence can be crucial in helping you prepare for counselling and the surgery that follows.
Grade III
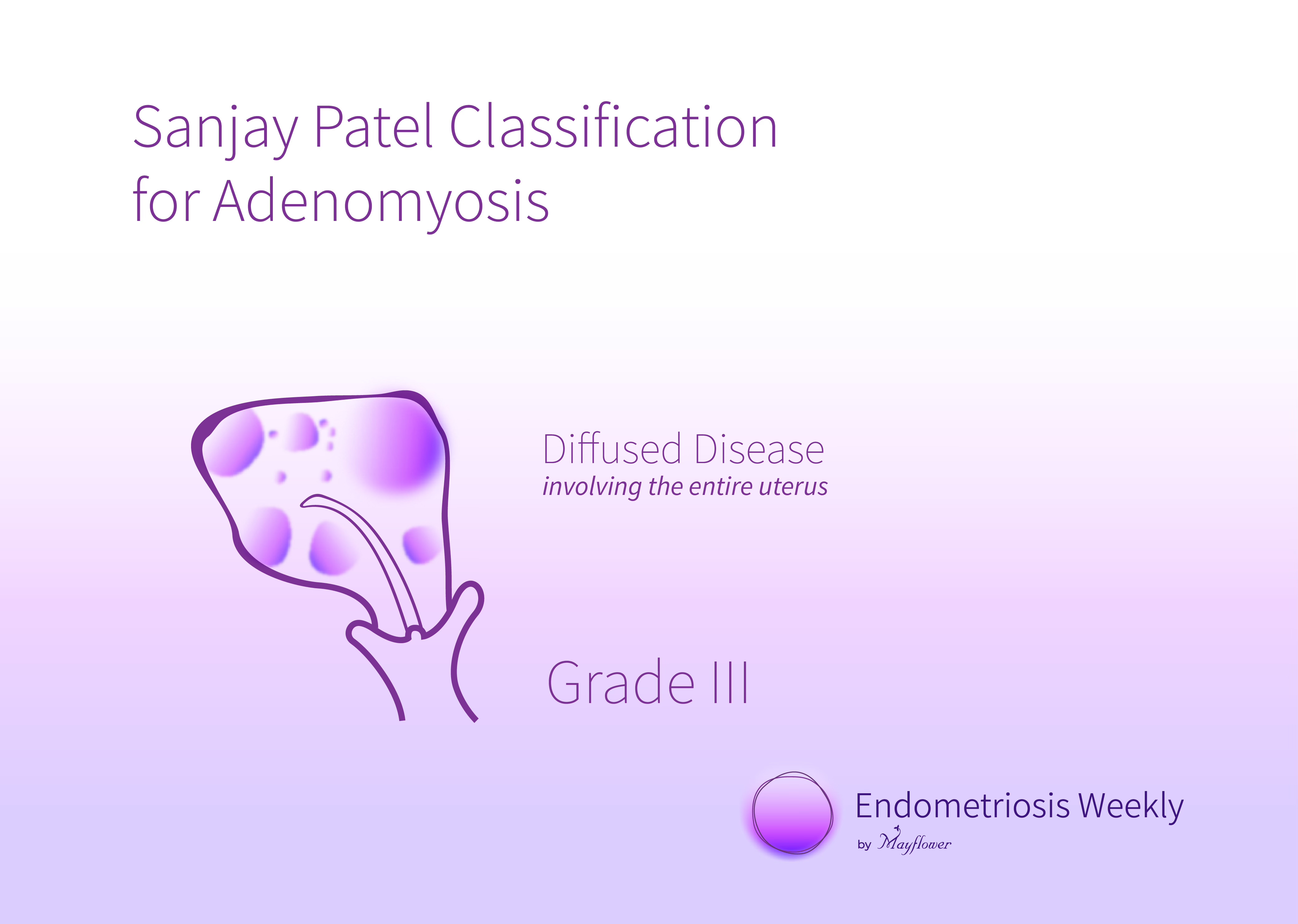
This is where the disease has completely taken over the entirety of the uterus. All of it is diffuse, densely vascular, and generally very hard to detect.
It’s that simple! This classification effectively characterises the disease along the two axis of occurrence; the size of focal masses, and the spread of diffused disease. This aids us in understanding what part is easily resectable and therefore opens up a wide range of choices for the procedures we can conduct.
Next week, we’ll return to our classification, and understand how various dissection techniques can help treat various incidences of the disease.
Until next time!
 | A guest post by
|
 | A guest post by
|
This new classification system is a simple yet powerful guide to decide the operability or to decide which ones are to be managed conservatively or surgically in my humble opinion. Kudos to Dr Sanjay Patel. Always a great fan of yours. I passed out my graduation and post graduation from Jamnagar, so I have a close association with anything from Gujarat.