



The Prisoner's Dilemma of Endometriosis Counselling
An intriguing phenomena shaping fertility and pain management procedures in endometriosis


Hello, doc! Today we unearth an interesting phenomenon taking over counselling for endometriosis. And it may have something to do with economics. But to understand that, you must first play a game.
A game with me, the writer. I promise it will be short, and I promise it will be fun.
Somewhere in a magical land far away, we stand facing each other and between us are 6 solid bars of gold locked inside a transparent box.

To open the lock, we must play a game.
Right next to where we stand are two buttons. Two on your side, two on mine.
One button says “snatch”, and one says “share”

To unlock the box, we must each press a button. We can only press one button, and we only get to press it once.
Now here’s how the game works.
If both of us press share, the box unlocks. Three bars float toward me, and three float toward you.
If both of us press snatch, 4 of the six gold bars disappear. Only one floats to you and the other one floats to me.
If I press snatch and you press share, I get to keep 5 bars, you get none.
Likewise, if you press snatch and I press share, you get to keep 5 bars and I get none.
Here’s a diagram to explain this.
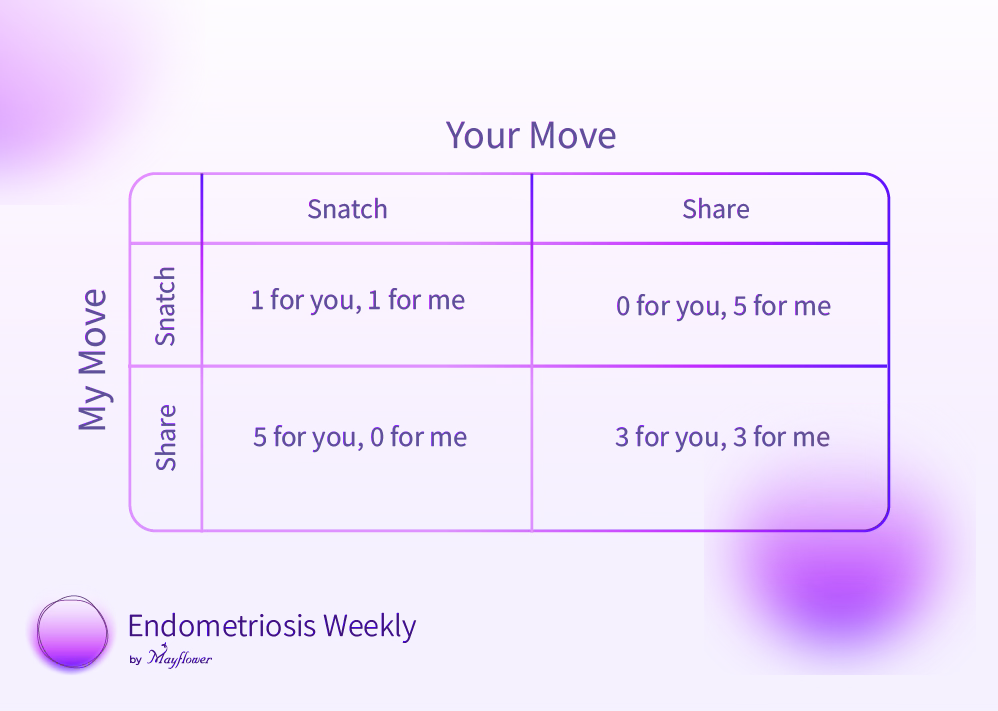
This is what economists call the prisoner’s dilemma. If both of us agree to cooperate, or in other words, hit share we gain the most. If both of us hit snatch we go home with very little. If one of us hits share, but the other hits snatch, the one hitting share is the sorry loser.
So, what button did you press?
When it comes to treating endometriosis, a lot of doctors have been choosing to snatch. Let’s understand what that means.
Patients generally don’t experience a disease, they experience a symptom. Or several symptoms. Which is when they reach out to a doctor and we record this as a “chief complaint”
The single goal of medical practice pivots around treating the chief complaint. And a caveat to be careful of the likely side effects.
In India, for patients diagnosed with Endometriosis, chief complaints are primarily of two types. 1) Absence or lack of natural fertility and 2) Cyclical or chronic pain
An ultrasound is enough to confirm that endometriosis is present, which is then often followed either by IVF or by Leuploride / Dienogest-based medical management depending on the complaint.
Pregnancies with endometriosis pose critical challenges as they are immediately triaged as high risk, while most patients being opposed to surgery, hardly wait to explore if medically altering their bodies to behave a certain way will have a long-term impact.
Across 20,000+ surgeries for endometriosis at Mayflower, we’ve seen what long-term medical management can do to the disease. We spoke about this in a lot of our previous editions. We’ve also seen the unpleasant effects of IVF in cases of deep infiltrating endometriosis. It is common knowledge.
Surgery when surgery is due, and a complete removal of the disease in the first go, are critical in ensuring a healthy recovery.
But do the doctors suggesting alternate treatments know this? Certainly. Do they refrain from suggesting surgery anyway? Certainly.
Why? The Prisoner’s Dilemma
If doctors in various parts of the country choose to advise a patient to get surgery, they also live with the fear that she might walk across the road to a competitor, willing to advise what the patient asks for.
So they choose to press snatch. Treat the patient like a consumer whose demands must be met, and met in a way that maximises gains.
By now, you should be able to visualise what the share and snatch buttons inside a counselling room look like.
“When you’re holding a hammer, everything looks like a nail”
Understanding the disease and the damage it does to the body is critical in understanding the correct treatment that must be administered for it. While the medical profession continues to evolve, testing new levels of commoditisation every year, we must remember that lesser-understood diseases need more compassionate treatments.
What should we then do?
We believe that treatment must have the following goals and in this exact order
Improve Quality of Life - People suffering from endometriosis battle a lot more than just physical symptoms. They lose a quality of life they once held close to heart. Returning them that quality is the biggest purpose of treatment and rehabilitation. This goal defines everything we do next.
Decreasing Pain Scores - An ideal decrease is from around 7-9 down to 1-2 in case of cyclical pain complaints.
Decreasing Gastrointestinal (GI) and Genito-urinary tract Symptoms - Restricted bowel movements, dyschezia, and more. DIE can present a variety of non-specific symptoms across both systems which need to be combatted for a better life.
Fertility - When we’ve achieved an anatomical state as close to the pre-disease condition as possible, only then is it optimal to begin considering fertility.
Following a conservative, tailor-made, multi-faculty, well-diagnosed approach to treating the disease to rehabilitate life in itself helped us improve fertility scores across patients.
Of 617 patients studied between 2019 and 2021 at Mayflower in Ahmedabad, 276 (~45%) were able to conceive naturally following a fertility-enhancing surgery for endometriosis.
Even then, each day we learn something new about the disease, and we are thankful to doctors from across the world who choose not to jumble themselves up in the prisoner’s dilemma, who rise above and save the medical profession from the clutches of microeconomics.
 | A guest post by
|
 | A guest post by
|