



Rectal Shaving - The First Line of Defence
Against endometriotic involvement of the colon


Those of you familiar with this 1980 British sitcom Yes, Minister will also be familiar with some absolutely brilliant and hilarious nuggets of truth that the show often dropped.
Amongst those, this one is my favourite. A line by the minister in the show that goes, “The three articles of civil service faith: it takes longer to do things quickly; it's more expensive to do them cheaply; it's more democratic to do them in secret.”

It’s counterintuitive, but it feels only reasonable. Today’s story of colon endometriosis, follows a similar oddly counterintuitive thought, and we see how that unfolds in actual surgery.
It’s harder to do less surgery
That’s right. It takes time to do things fast, and it’s harder to do less surgery. Often when the colon is involved in endometriosis, surgeons find it easy, or dare I say, convenient to follow a more radical approach to surgery. In last week’s edition, we detailed out the Rule of M, a decision making framework we follow decide what procedure to follow in what case of colon endometriosis.
The following two images serve as a quick recap to that idea
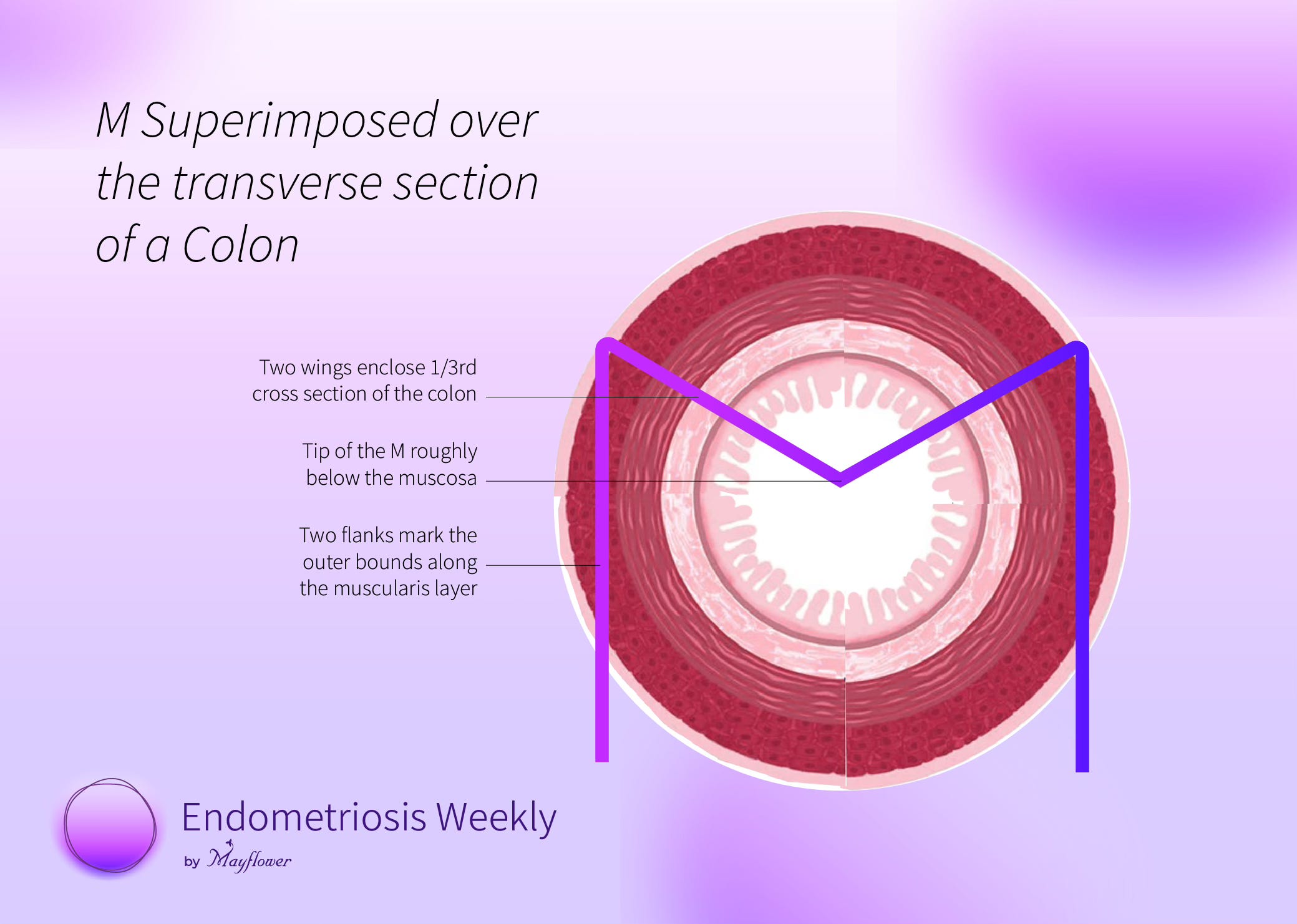
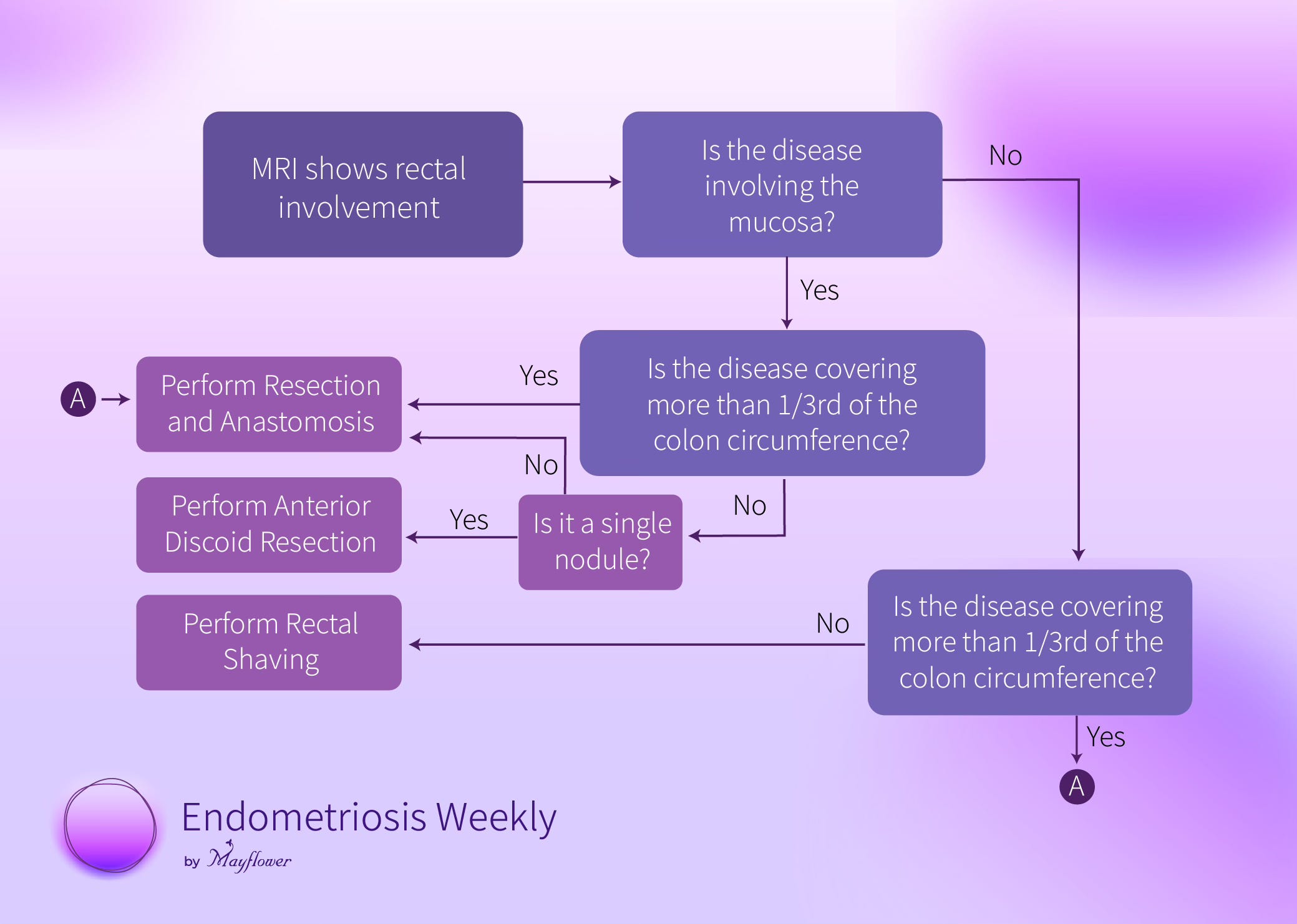
You can notice from the flow chart above that the circumferential involvement and non-invasion of the mucosa are key factors in deciding whether shaving can be performed at all.
The larger purpose of this rule is to see where resection can be avoided
To that end, the framework heavily depends on the circumferential involvement of the disease on the colon. If a nodule isn’t invading the mucosa of the colon, there is actually no need to conduct resection an anastomosis, not matter how far the nodules might be spread along the length of the colon. But if circumferential involvement exceeds a third of the colon, resection remains to be the only option.
To understand why, we must first look at the 4 steps of conducting rectal shaving.

This is a case from some time ago. The nodule is showing a serosal and subserosal appearance on MRI but isn’t invading the mucosa. The best way we know so far to excise it is as follows
Step 1: Split the nodule
Split it along the recto-vaginal plane staying as flush to the fat of the colon as possible. This will send a large part of the nodule towards the uterus and you know how to deal with that.
Step 2: Denude the fat
Slowly, but surely, bit by bit, denude the fat from the nodule, giving you a clear margin of its actual existence. Being careful, slow, and precise is more important than anything else in this step. At the end, you will have a clean outline of the nodule.
Step 3: Pop it up!
The nodule is imparting compressive stress to the colon. You can only visualise the top of it and major pathology lies beneath the surface but if you want to excise it without perforating the colon, proceed slowly, use the tip of your ultrasonic scalpel snip gently on different points of the surface and this will slowly pop the nodule out.
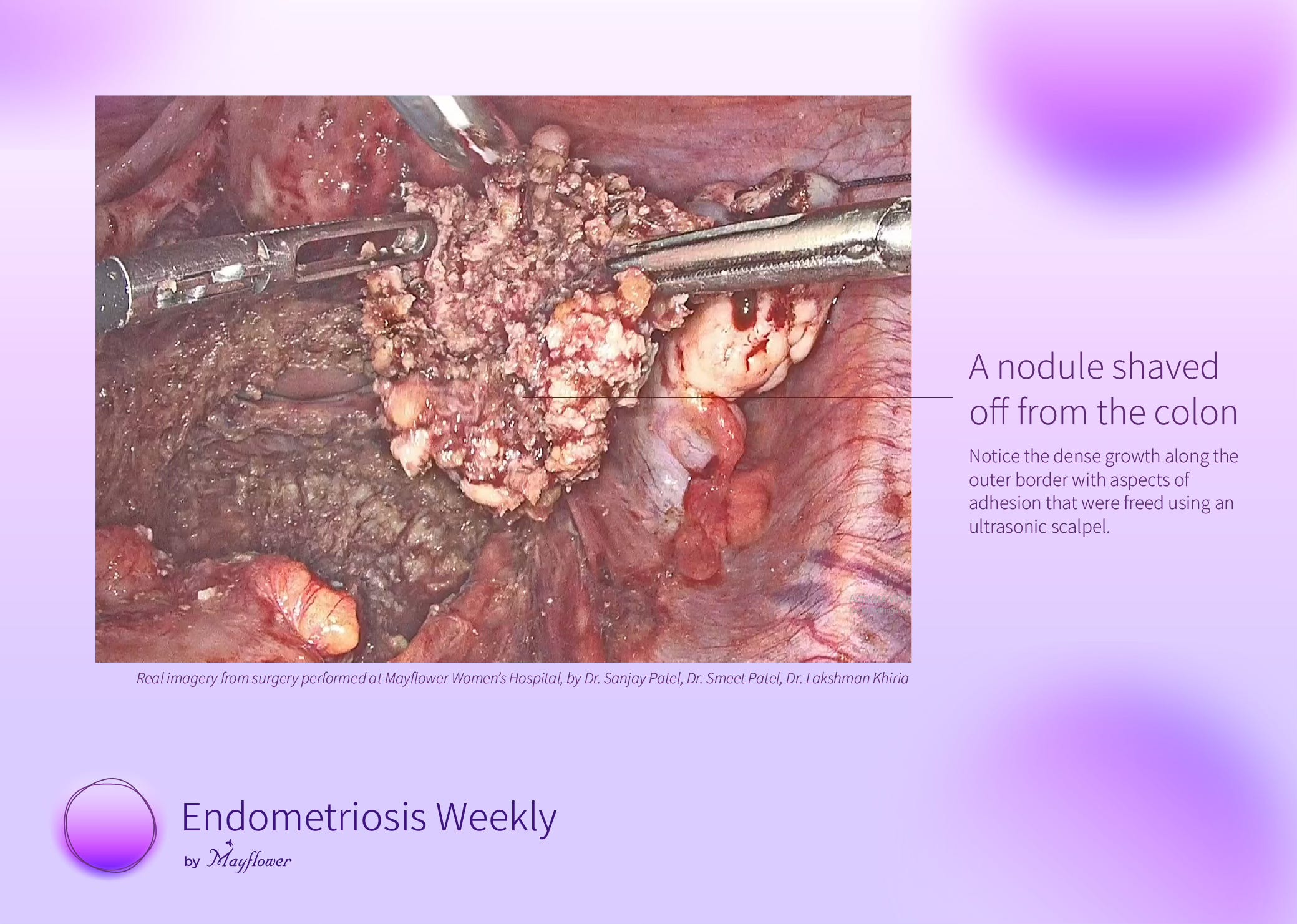
Step 4: Shave it off!
With the tense adhesions out of the way, careful shaving towards the invasive part of the nodule will free it from the colon and you will have with you a beautiful, single block, excised nodule.
Now let’s come to why 1/3rd. It’s a simple physical limitation explained in this badly made drawing.
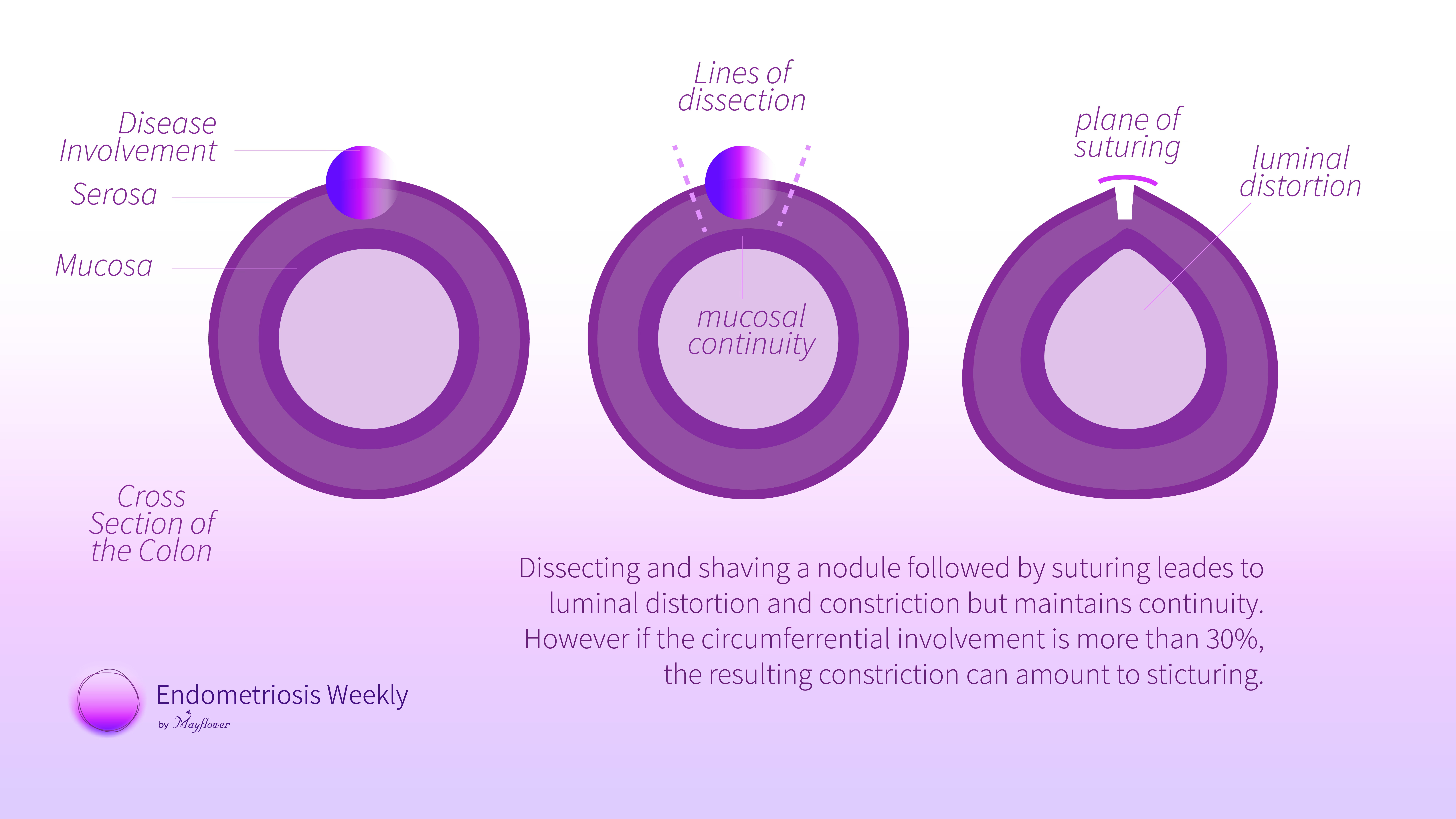
Dissecting and shaving a nodule followed by suturing leades to luminal distortion and constriction but maintains continuity. However if the circumferential involvement is more than 30%, the resulting constriction can amount to sticturing.
The constriction begins to limit colonic function and that’s when we’re left with no option but to excise a longitudinally a section of the colon through a resection and anastomosis procedure. The biggest drawback there is LARS or the Lower Anterior Resection Syndrome, a combination of dysfunctions that really cause havoc in a patient’s life.
The Rule of M therefore has proven to be an easy and effective tool to triage patients based on the findings form an MRI and help them undergo a surgically more difficult, but less invasive, and less radicle surgery that shows consistently lower recovery and rehabilitation time helping women go back to a life they once left behind.
But before we go, a quick reminder. CSEEMIG’s 14th batch is about to begin soon. If you haven’t grabbed your seat yet, do it soon. I promise you it’s the most fun you’ll ever have learning surgery.
It’s the middle of May and some of the best mangoes of Gujarat will be around at the time. You don’t want to miss those either.

And we get to meet one on one! Couldn’t get any more fun than this!
That’s it! We’ll see you next week.
 | A guest post by
|
 | A guest post by
|