



Pain in Fine Print: Understanding the Emotional Cost of Endometriosis



I’m about to share with you an idea that set me off thinking for a long time when someone first said it to me.
Cost is often understood in action but rarely in omission.
What does it mean? We are trained to understand the idea the cost of doing something. Buying petrol will cost you something, as will buying onions, as will getting a new car. Doing something has a cost. We are therefore brought up, in most Indian households, to do as little as possible because the more you do the more it costs.
Rarely does someone talk to us about the cost of not doing something. Except for if you are a parent (study, or you will grow up and sell vegetables) or a kidnapper (give me the money or your child dies)
But besides that, not much gets told to us about the cost of not acting. Let alone the non-financial costs. More than the pain of a disease like Endometriosis, it is the non-acknowledgement of all its costs that burden the women who live with the disease. In today’s edition, we look at the emotional cost of endometriosis and the deep scars it leaves on women, especially when they choose not to act on it.
The impact of endometriosis on a person can be described as a dark never ending chapter of their lives. A chapter through which they feel completely broken. Feel as though all their dreams are shattered. And where even a basic activity like having tea in peace feels like an impossible task.
From the moment one first experiences severe pain - the clearest symptom of endometriosis - the victim has zero idea why it is happening, let alone how much their life is about to change along with their mental health, relationships, career, sleep, self worth, and less importantly yet considerably, their fertility.

The Pain Stories Project documents in significant, graphic, and elaborate detail, the suffering of those who chose to speak up.
“Like torture. Like somebody is gripping, squeezing, cutting, prodding, stabbing you inside, and won’t let go. The waves of pain last for so long you can only take some painkillers, curl into a ball, and cry yourself to sleep.”
“It’s a full body experience for me. It starts as a dagger being stabbed in and moved around in my womb. That’s the most acute part. Then it feels like the blood is draining from my legs and face. My whole body aches.”
You can read more of these on The Pain Stories Project
But as professionals who deal with patients on a daily basis, empathy is a bare necessity, but empathy alone is not enough. We must understand what factors of life contribute most to the emotional cost.
The first step there, is making a list. Of all the things that levy an emotional cost on a patient of endometriosis. One dimension of emotional cost is its visibility. Can you clearly see them in pain, or in distraught, or are they hiding it? Can you tell that they are emotionally turmoiled, or is that a part of their lives you simply don’t know.
On the other hand, there is the dimension of direct cost. Over reliance on pain medication, and strained relationships at work and in family levy a high direct cost but may or may not be visible, at the same time, aspects like low fertility don’t have a direct cost on the patient but its visibility within family and society can be discouraging and straining.
These two dimensions help us categorise problem, symptom, and root cause discovery as professionals.
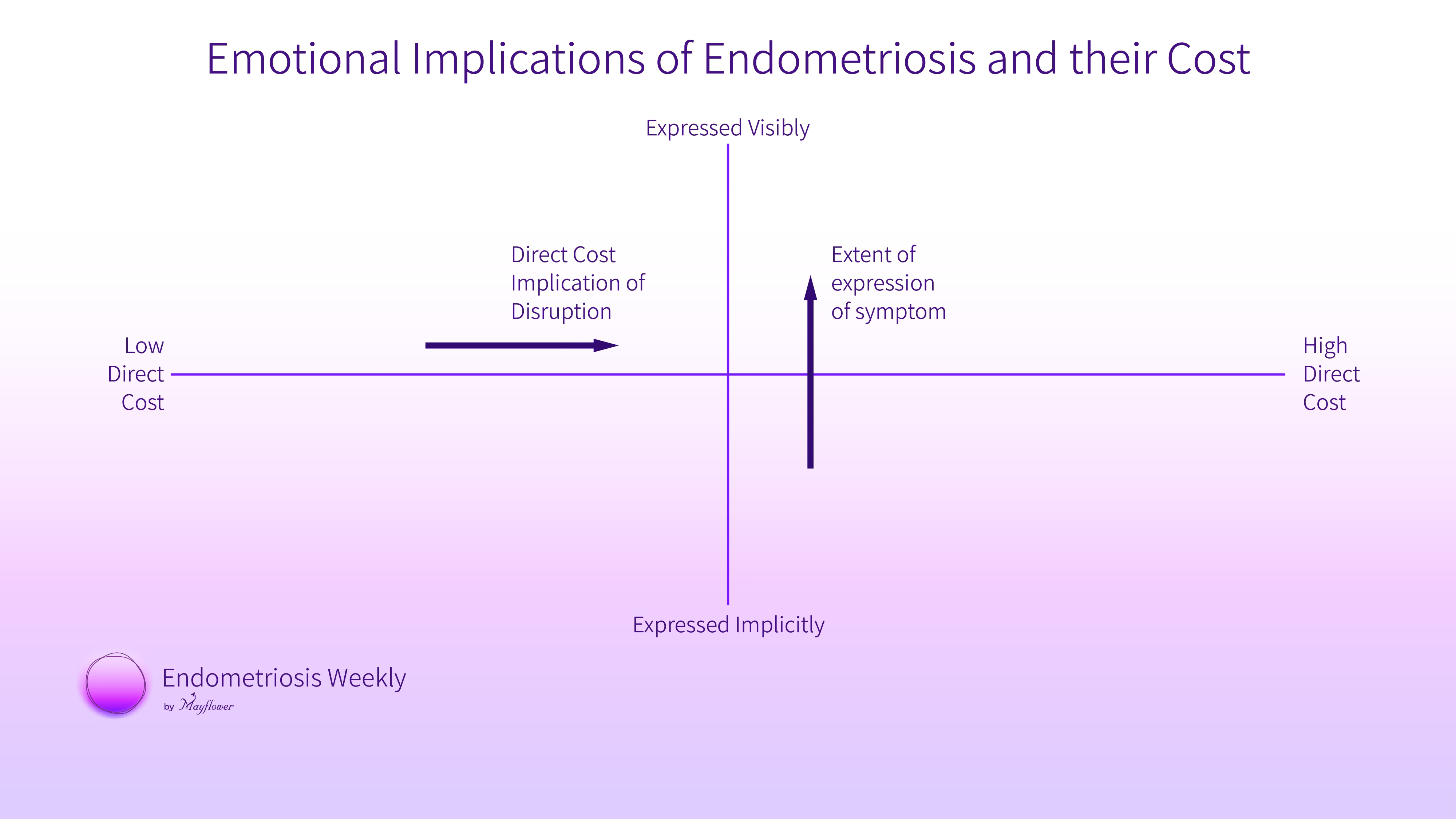
One the one axis we lay the cost, on the other, explicitness of visibility.
Laying out some problems, this graph begins to show us an interesting picture.
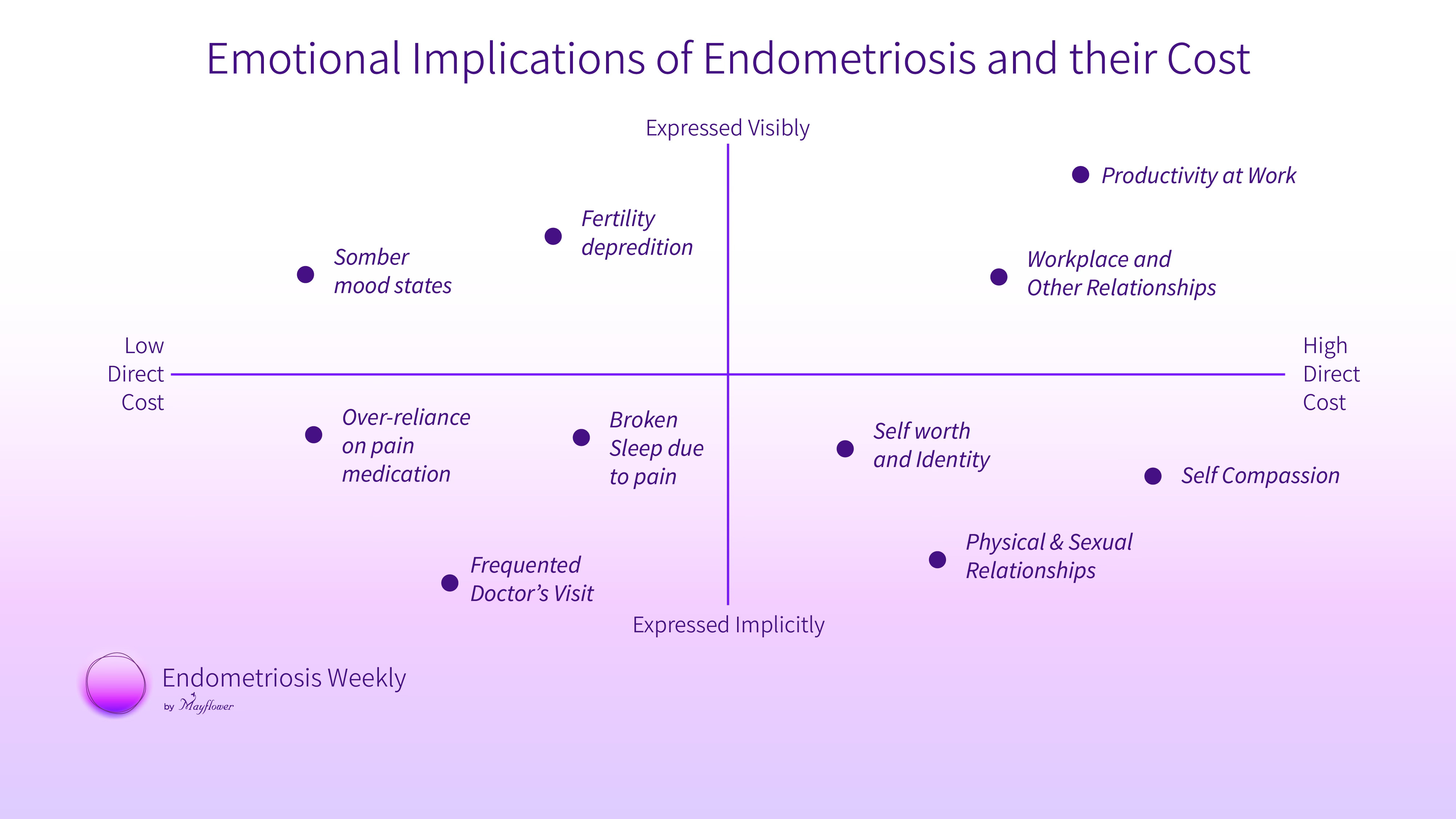
Low productivity, strained relationships, fertility, and mood states might be very visible, but often their relative costs get misunderstood. Low productivity at work, the inability to lead a normal life clearly has a much higher direct cost compared to being deprived of fertility. Yet, we have sprawling empires built on top of IVF but little for post surgery rehab.
Similarly, aspects like frequent doctor’s visits can and will be invisible to most people around a victim of the disease as will the strained sexual relationships but they come at a great cost of frustration, of a loss of personhood, and identity.
What can we do?
There isn’t one clear answer, but there are some directions.
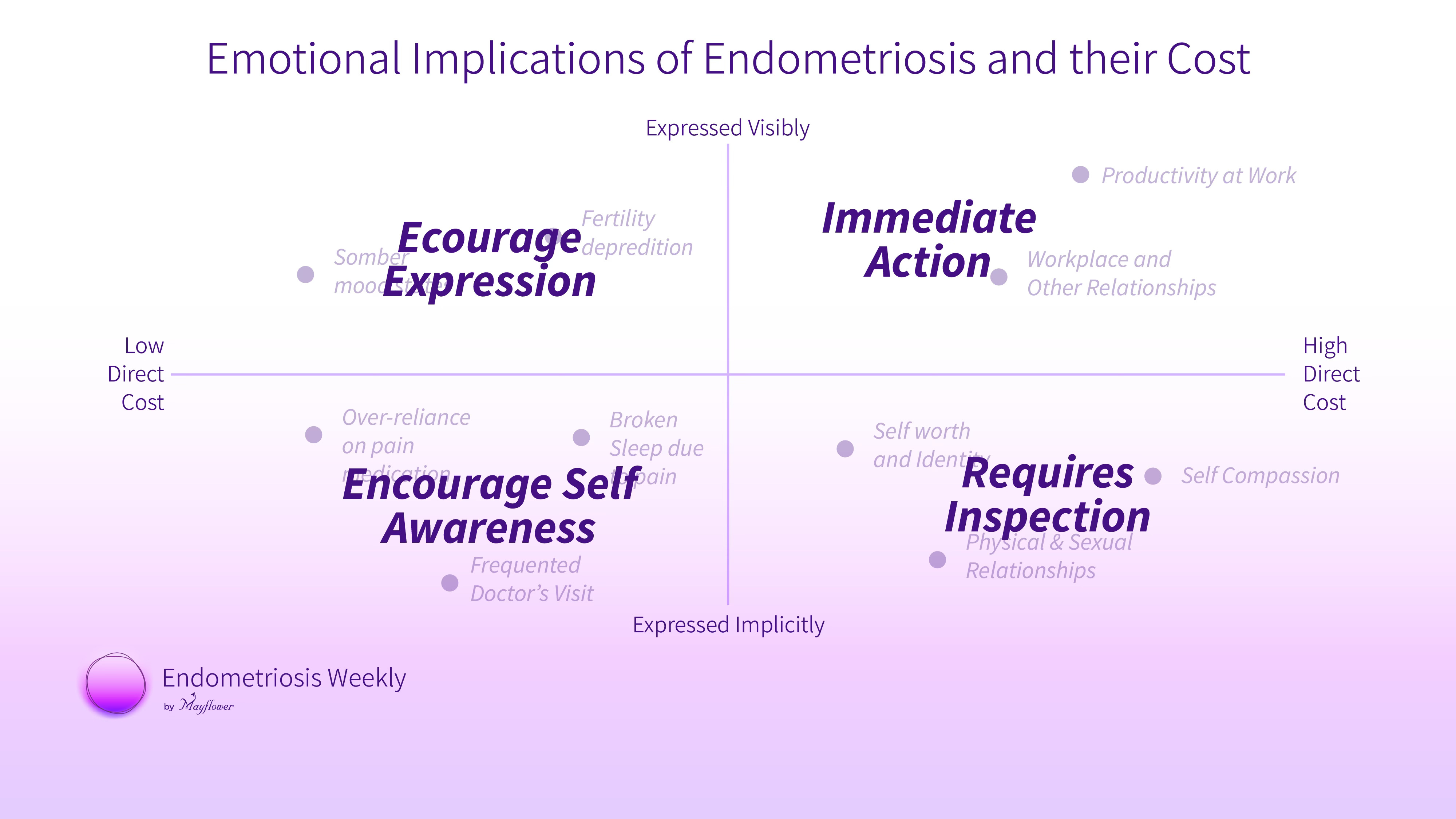
If the problem has a high visibility and a high direct cost, it needs to be treated right away. This is also why we keep stressing how important the first surgery for endometriosis really is. Restoring normal life is the first step towards solving all the other problems that come with it.
Problems with high direct cost but low expression need inquiry. Over time, each of us as medical practitioners have found a radar to look for these problems that patients might not directly inform us about, but nonetheless, we know they might be facing. It is now our responsibility to create spaces and options for patients to share them with us more openly. These are the problems fixing which will cause the highest amount of benefit to the victims and the society.
Problems with low expression and low direct cost are sometimes self manageable, and some other times a consequence of inaction. Making the right choices, or becoming more aware of the condition and its implications can greatly help patients find a new grounding. A well understood pain, hurts less.
Widely expressed but low cost problems are a great opportunity for expression and conversation. These are the drivers that can get most people to converse about that conversation and bring out more of the less expressed symptoms and costs of the disease.
That’s the lay of the land. By no means is it wholistic, but it certainly is a great place to start. Before anything else, it’s a place for us to acknowledge that there exist costs to not performing a total, complete, anatomically restoring surgery. There’s a cost to not doing what is in best interest of a patient. And the cost is human life.
We will see you next week.
 | A guest post by
|
 | A guest post by
|
 | A guest post by
|