



Managing Adenomyosis: The Hood Technique
Steps, tips, directions, and more


Last week’s edition on the elliptical technique for managing adenomyosis got some significant interest from doctors all across the world. So we decided, it was only fair to double click on the moment and dive a bit deeper into the management techniques.
The second most commonly used technique for managing adenomyosis is the Hood technique. It is especially useful in cases where the adenoma is deep seated and the serosa of the uterus is free from the adenoma. Today’s edition takes a close look at the steps involved in performing the technique.
The hood technique is very similar to the process we follow in a myomectomy surgery but the procedure differs in the sense that we dont’t get clean and definite planes of dissection as in the case of a myomectomy surgery.
It’s more similar to digging into the uterus to find the adenoma, and then scooping it out almost.
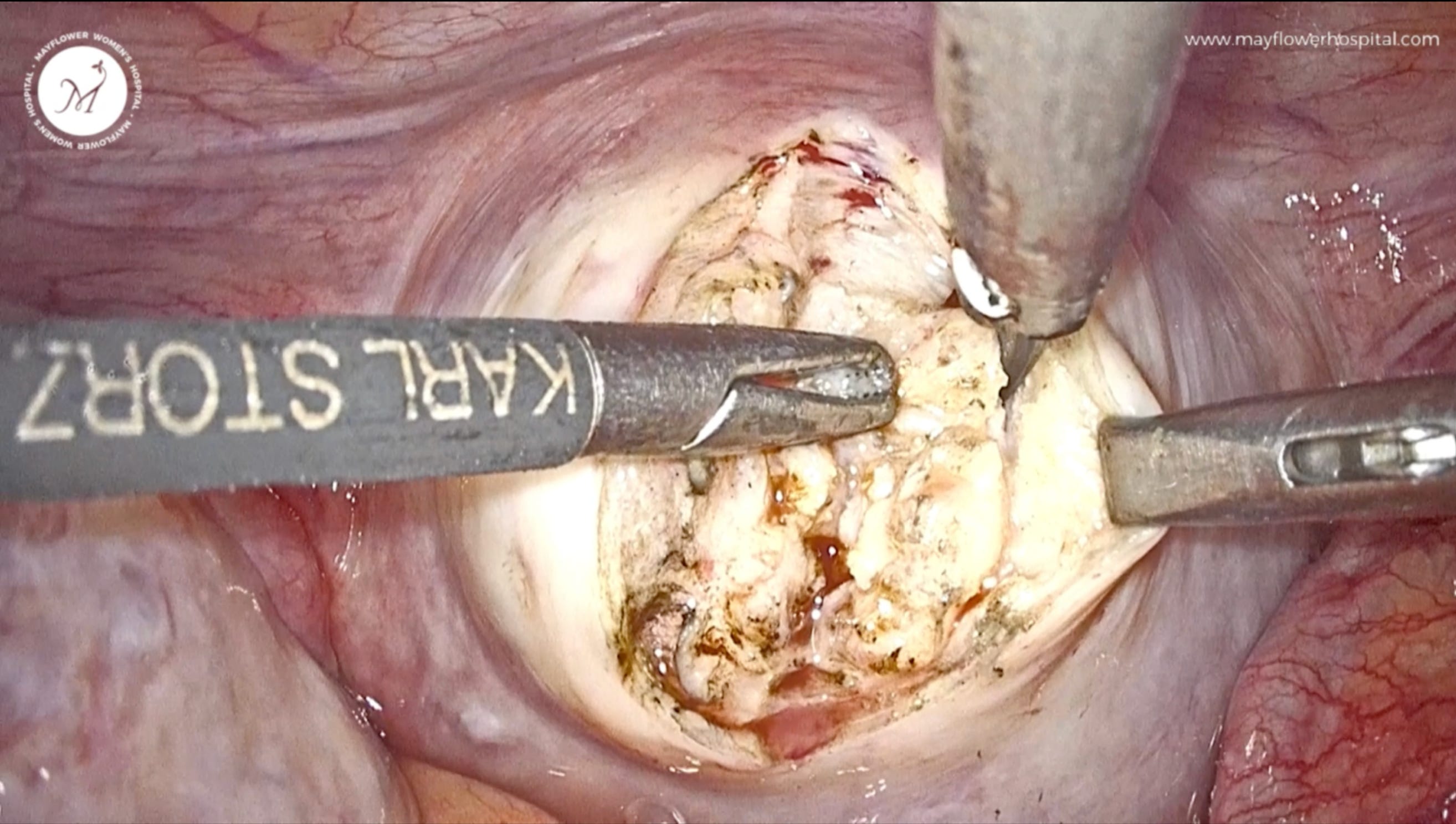
The process begins with placing a midline incision first. As the incision is deepens you will be able to see and feel the margins of the adenomayotic tissue. The tissue texture is puckered, and dense, and unlike a fibroid, this doesn’t simply pop out.
So we go around the facia of the adenoma within the uterus and detach it from the walls, akin to digging it out of the uterus.
The texture of the tissue and also where it is placed, makes most of the challenge. But the learning curve on this is not steep at all. Once you get used to the texture and how it reacts to different instruments, it is only a game of patience.
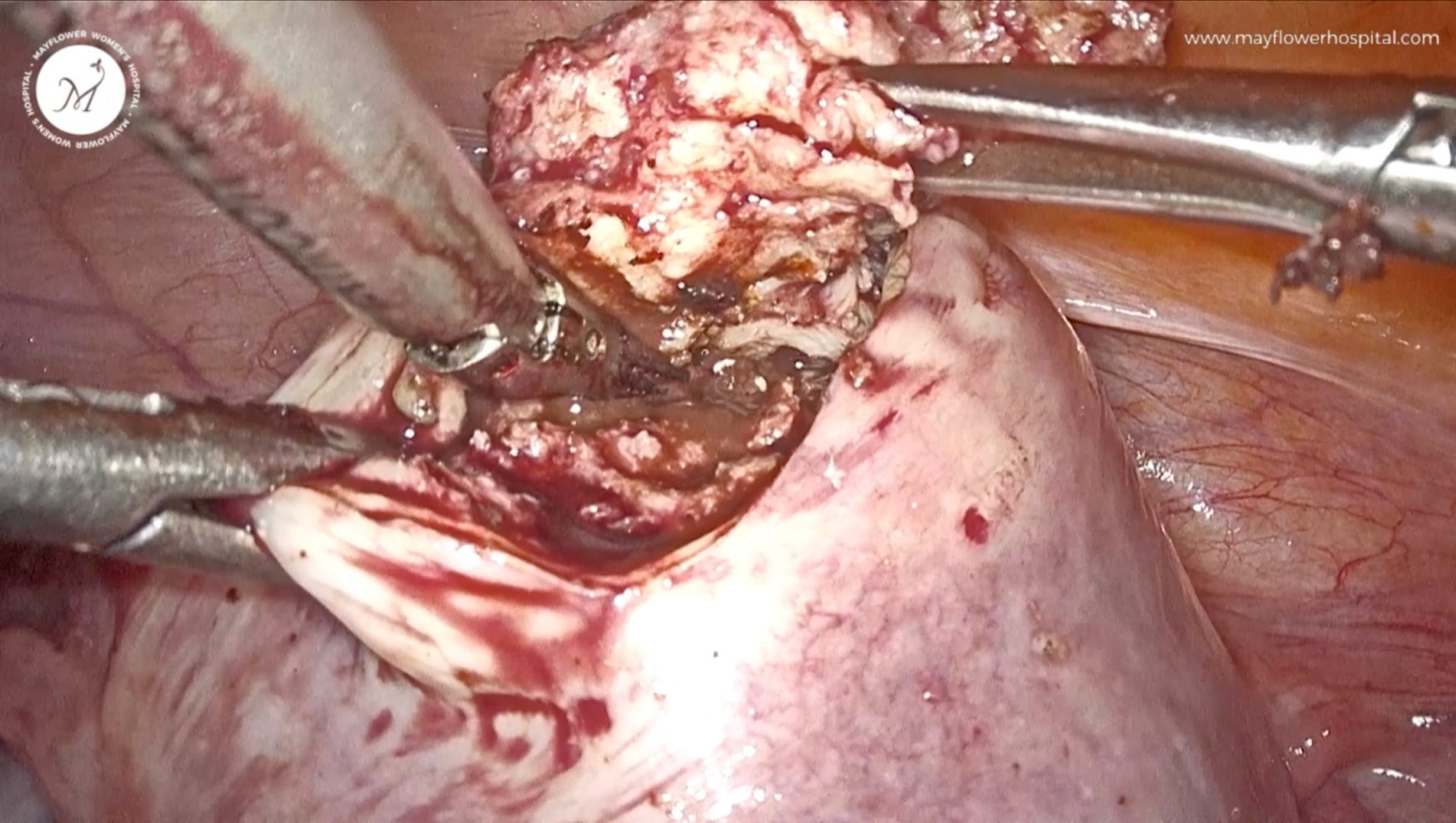
Like in most cases, the adenoma isn’t highly vascular. You should encounter minimal bleeding while dissecting it. Anyhow, if you do encounter stronger bleeding you should know that you’re probably digging into health tissue. At that point, it’s advisable to retreat, settle any major bleeding and then begin again with greater caution.
Once done, you should have a clean adenoma between your graspers. Because of the fundamentally different nature of the tissue, its margins are clearly defined compared to more healthy uterine tissue.

Another aspect to be careful of are cystic appearances. Similar to what can be seen in the image below, cystic collections are a source of chronic pain and other grave symptoms like dysmenorrhea. Removing them in totality with not residue left behind is important to ensure a total post-op recovery.
Suturing for the most part is the same as we discussed last week. And that’s it. That’s the technique. It is simple, rests on few basic principles, and is quick. But it holds significant curative power in terms of symptom alleviation and fertility enhancement.
We’ll keep it short this week. Hope you have a good one!
 | A guest post by
|
 | A guest post by
|