



How does Endo Happen?
A fresh conjecture on disease propagation


How does endometriosis occur? It’s been a question froth with intrigue especially given how its occurrence has recently seen an uptick.
There are four major schools of thought or theories of how/why Endometriosis occurs. This edition talks about the fifth.
But before we jump to the conjecture on why this might be happening, let’s do a quick recap on the four other theories:
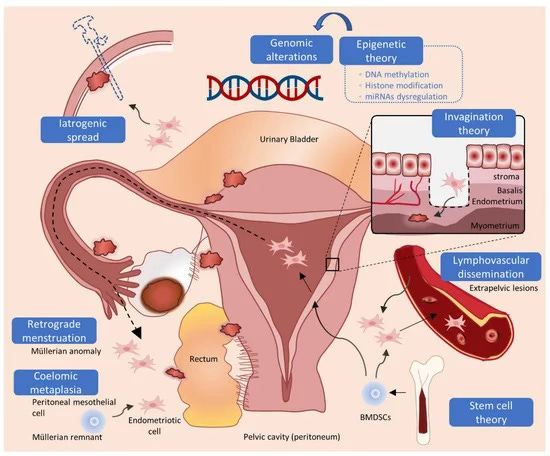
Retrograde Menstruration: Most commonly accepted idea where we suggest that endometrial tissue sheds within the uterus and moves backwards through the fallopian tube making its way into the pelvic cavity. It’s what most people believe to be true.
Coleomic Metaplasia: a lesser known but significant theory that refers to metaplasia or an unwanted transformation in the colonic tissue leading to endometrial growth that then further spreads to the rest of the cavity.
Stem Cell Origin: a more predicatable but less consensus gathering theory that suggests that cells responsible for the regeneration of the endometrial lining play a role in the development of endometriosis. The spreading of these stem cells to ectopic regions may then lead to the differentiation of endometrial cells and eventual endometriosis.
Mullerian Agenesis: The most interesting of all, this theory gives endometriosis a congenital colour and suggests that the leaving behind of cells during the merging of the mullerian ducts at the time of development of the Genito-urinary-tract is the primary cause of endometriosis.
To understand the 5th conjecture of endometriosis origin, we must first go back to what normal anatomy looks like. Here’s a quick sketch.

This system consists of the vagina, uterus, fallopian tubes, and the ovaries. Next to, and all around this system are critical as well as branched out blood vessels that carry essential fluids back and forth.

The aorta branches out in the common illiac artery on either side, which further breaks down into the internal illiac artery and exerternal illiac artery. The internal illiac further then branches out into the uterine artery which reaches up to the uterus from over the ureter, that connects the kidney to the bladder resting above. (remember water under the bridge)
Now while any of the 4 theories could have led to the occurence of endometrial tissue outside the uterus, here is how we think the propagation might work.
Step 1: Growth
With each cycle, the tissues growth under the influence of hormones (GnRH, LH, FSH, and so on). This is parallel to the growth of the functional endometrial linning within the uterine cavity and because the cells of endometriosis are similar if not the same as the cells growing inside the uterus, they too share similar patterns of growth.
Step 2: Shedding
As the cycles progresses, the tissue sheds. From within the uterine cavity the tissue simply flows out, however in the pelvic cavity it has nowhere to go. It stays there. As it is.
Step 3: Fibrosis
On the other hand, it gets picked up by the immue system as a misplaced but not-foreign tissue. Our immune system simply causes an apoptosis of the tissue, leading to fibrosis, with the goal to contain the cell growth.
In a subsequent cycle the growth begins again, the shedding follows, and finally ends in fibrosis. This explains why endometrisis tissues display a layer by layer growth when observed upon dissection.
Important Inferences
This conjecture of propagation explains how the disease might spread from one place to the other owing to shedding
It also explains how invasion into organs might happen owing to the vascular nature and needs of the endometriosis tissues.
This change in perspective makes clear the fact that the disease of endometriosis is a hormone dependent disease
However, the ectopic presence of cells and their fibrosis doesn’t stop growth or infiltration from happening.
Temporary supression of hormones is not a good solution to the problem. In a non-regenerative, or topologically dependent disease that might have helped but with endometriosis, it simply delays the problem.
A complete removal of the disease is critical. Leaving behind traces can also lead to recurrance in a very short time.
Medical management might have a post operative role to play in endometriosis but it is definitely not enough as a stand alone solution.
If you have thought around the observations you have had about the growth and propagation of the disease, please leave them in the comments below. We would love to read more about them.
That’s it for this week! See you again in 7 days!
 | A guest post by
|
 | A guest post by
|