



Endo's Tryst with the Appendix
Managing appendicular involvement in endometriosis


One of the easiest most common surgeries generally known is an appendectomy. You would know at least 5 people around you who had one, even if you aren’t a doctor yourself. But you are. And you probably know more.
Things get complicated however, when this appendix is involved in a case of deep infiltrating endometriosis. In this week’s edition, we take a peek at an involved appendix is handled, dissected, and removed.
The incidence of the involvement of an appendix isn’t common, but at the same time, it isn’t something that should take any of us by surprise. (recent studies have found endometriosis tissues present as far as the brain) Anatonimically, the appendix is situated at the cranial right corner of the pelvic brim. So technically, it’s still in the pelvis making it a ripe candidate for involvement, given the right conditions.
The pelvis is a pandora’s box, several systems come together when you operate in that region and if a total removal of the disease and a pain free post operative life of the patient is our goal, handling its involvement in all those systems becomes crucial.
This is also why a thorough pre-operative mapping of the disease, followed by the formation of a multidisciplinary team for the procedure is crucial in ensuring success. In this case, that crown rests heavily on the head of the GI surgeon.
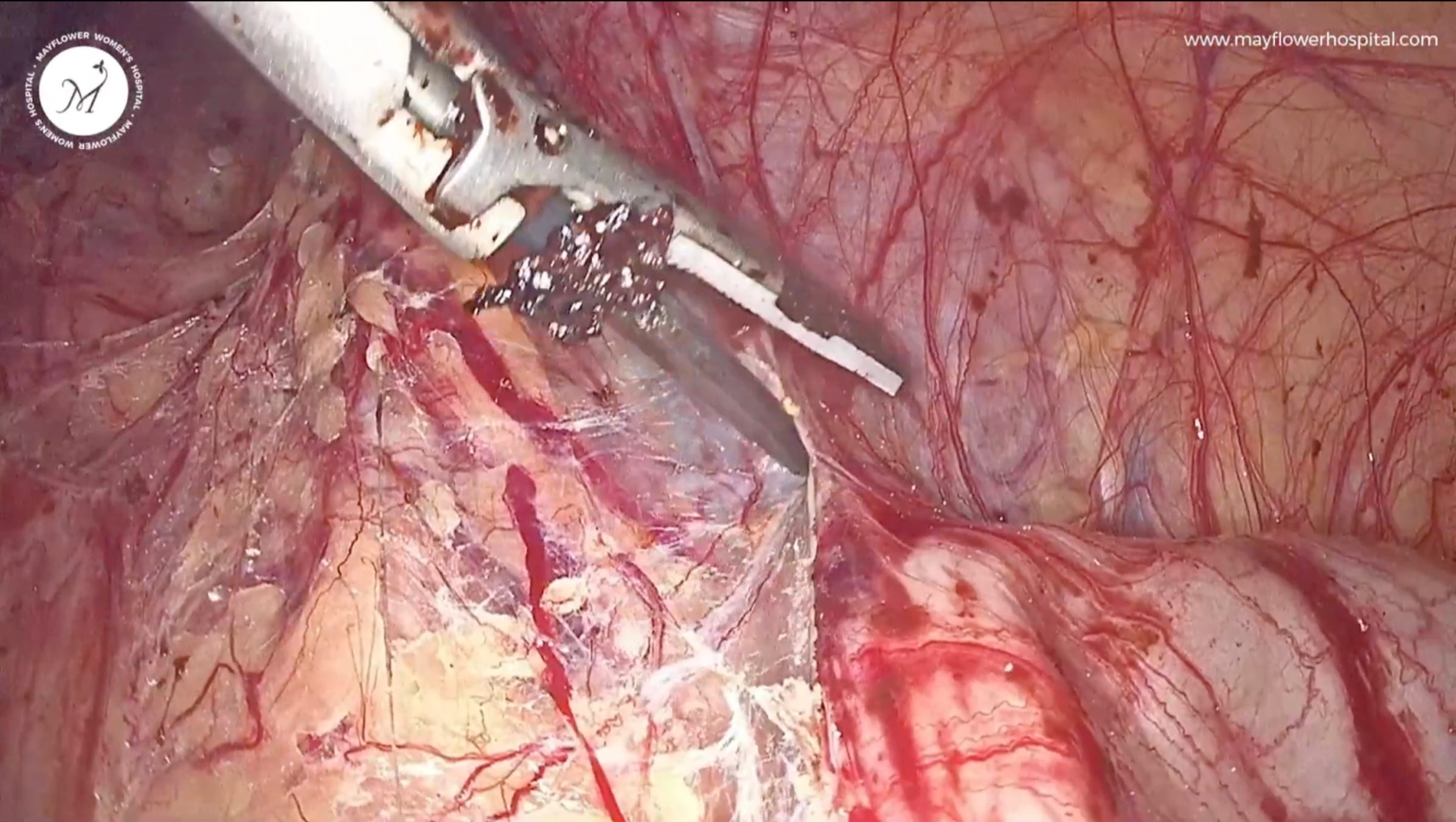
Getting right into the surgery, here’s what you will see when you first take a peek

Like in all endometriosis surgeries, we first remove the disease from all the other major sites of occurrence before proceeding for the appendix. Since the organ is still well within the pelvis, our port placement does not change. (You can read about our port placement methodology here
Step 1
We dissect the adhesions surrounding the appendix. The idea is to bring about clear margins for an eventual surgery. In this process, all the parenchymal tissues are taken care of.
Pro Tip: What helps the most when venturing into dealing with involved organs is the differentiation of tissue texture to tell them apart. Different tissues will react to your ultrasonic scalpel differently and create varying results depending on their relative collagen and elastin contents.
Step 2
Once we’ve dealt with the involvement, we attend to the mesoappendicular part. This is where every surgeon must be careful. The region is highly vasular so a proper coagulation is necessary when proceeding with any dissection. For times like this, the advanced bipolar comes in handy because of it’s ability to vary current pattern basis tissue type thereby creating a more effective seal.
Step 3
Now all the parenchymal tissue is dissected off till the base of the appendix; essentially speaking, we’ve made the appendix naked and ready for removal.

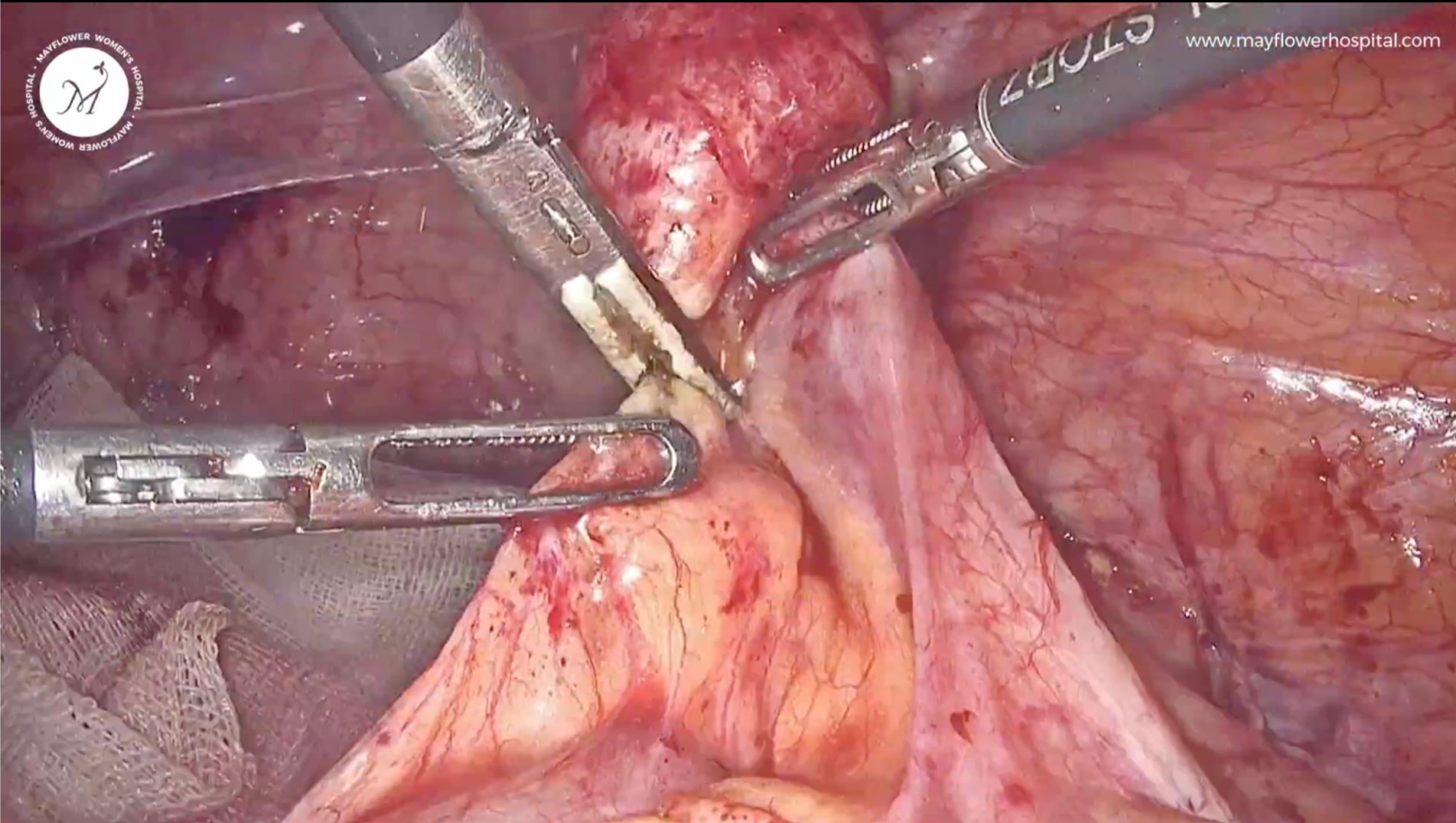
Step 4
Constriction is done using two free ties. We use 2/0 vicryl ( polygalactin 910 ) for the first free tie. 2 throws are made, and the entire structure strangulated; all the while making sure that we don’t tear the appendix.
Following this, an overthrow is made and a surgical knot is achieved. 2 of such throws are made.

This is what the constricted ready for excision appendix looks like. We dissect this mass and deliver it out bidding it farewell into the histo-patho lab. Then we go right back to where we left things off and check for homeostasis, before making a final exit.
That’s it! That’s how we handle an appendicular involvement of endometriosis.
Hope you had fun reading this. If yes, please share this with your friends!
 | A guest post by
|
 | A guest post by
|