



Disease in Breach: Treating mucosal disease involvement on the colon


The air is thick with the kind of news we’ve been hearing this past week. It’s hard to start writing without acknowledging just how difficult it must have been for a lot of us to navigate through life this past week. Our heart goes out to the families of the bereaved and injured. Every nation finds itself in times where it must meet what it’s made of. This is our time.
With that backdrop, let’s dive into our edition for today.
Last week we discussed how rectal shaving presents an efficient, efficacious, and preferable alternate to resection and anastomosis in cases that qualify. This week, we will dive into anterior discoid resection, a second alternative procedure that maintains neural connectivity in the colon while also leading to a total removal of the disease.
But before we do that, it’s important that we do a refresher for Mayflower’s Rule of M. As you might know from our last edition, we overlay an M on top of the transverse section of the colon and map the disease.
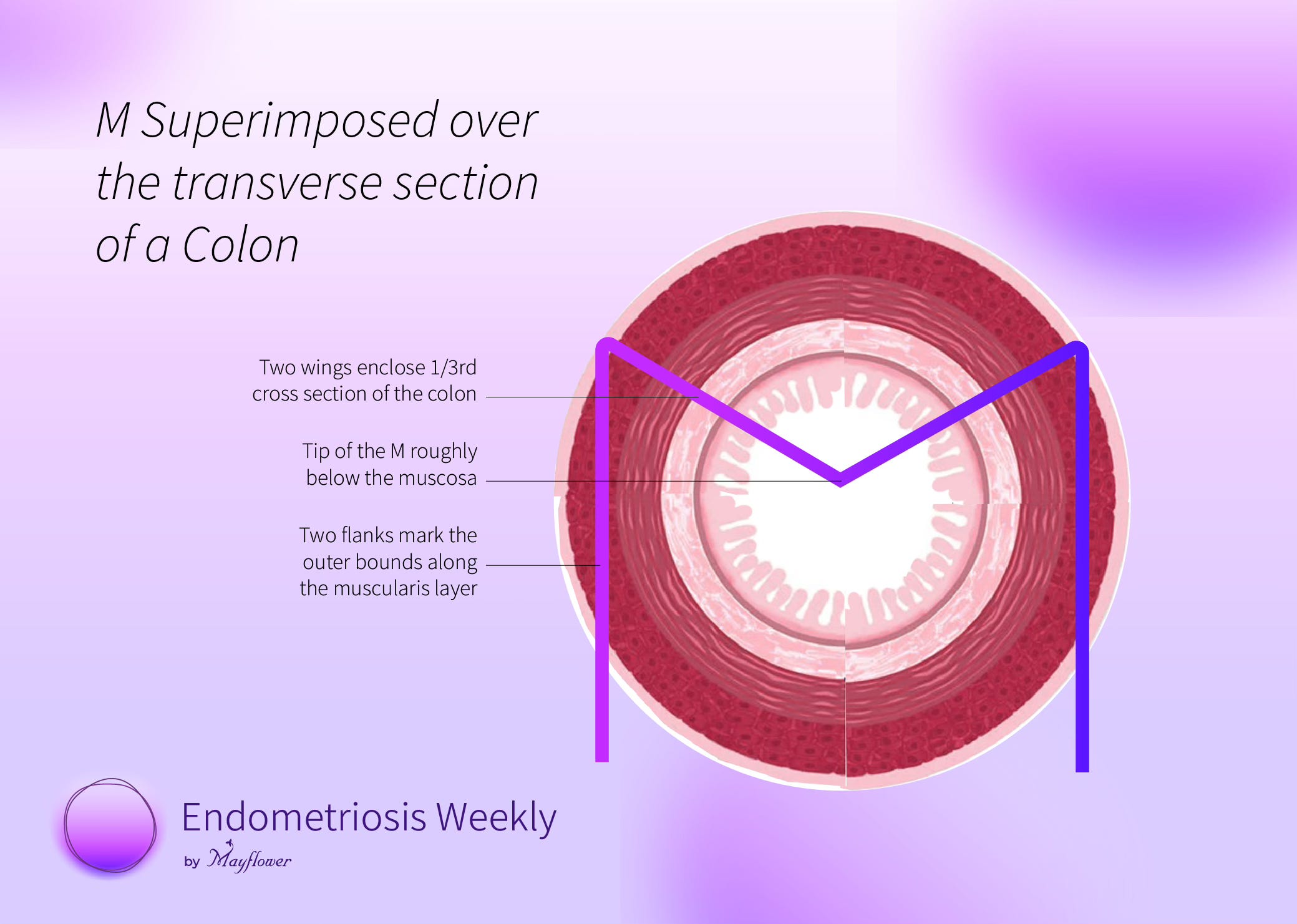
Based on how the disease infiltrates radially and spreads peripherally, we can make a decision on what procedure to perform using the following framework.
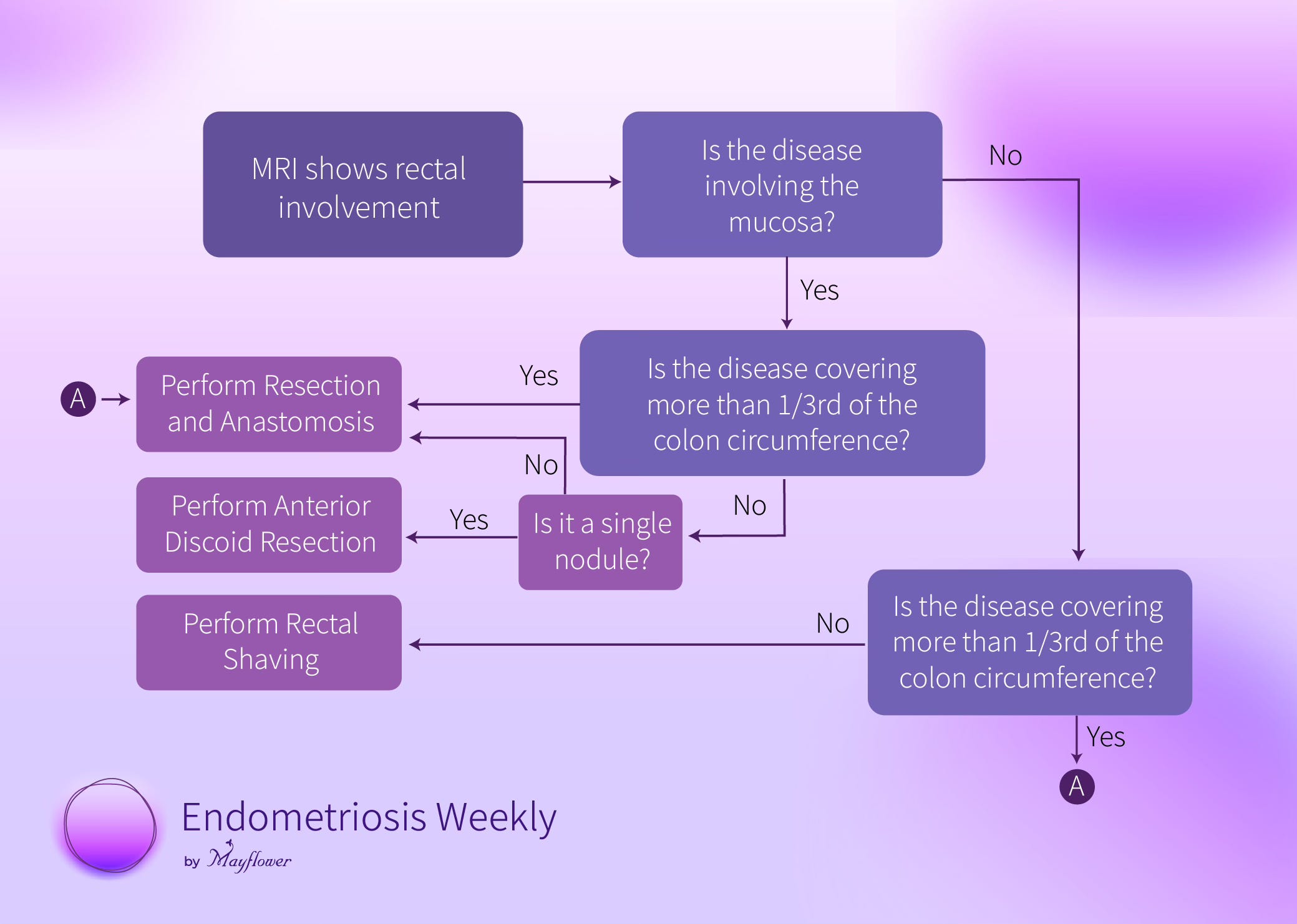
It’s easy to see here that ADR (anterior discoid resection) is something we perform when the mucosa is involved, the disease doesn’t cover more than 1/3rd of the circumference, and there is no more than 1 nodule.
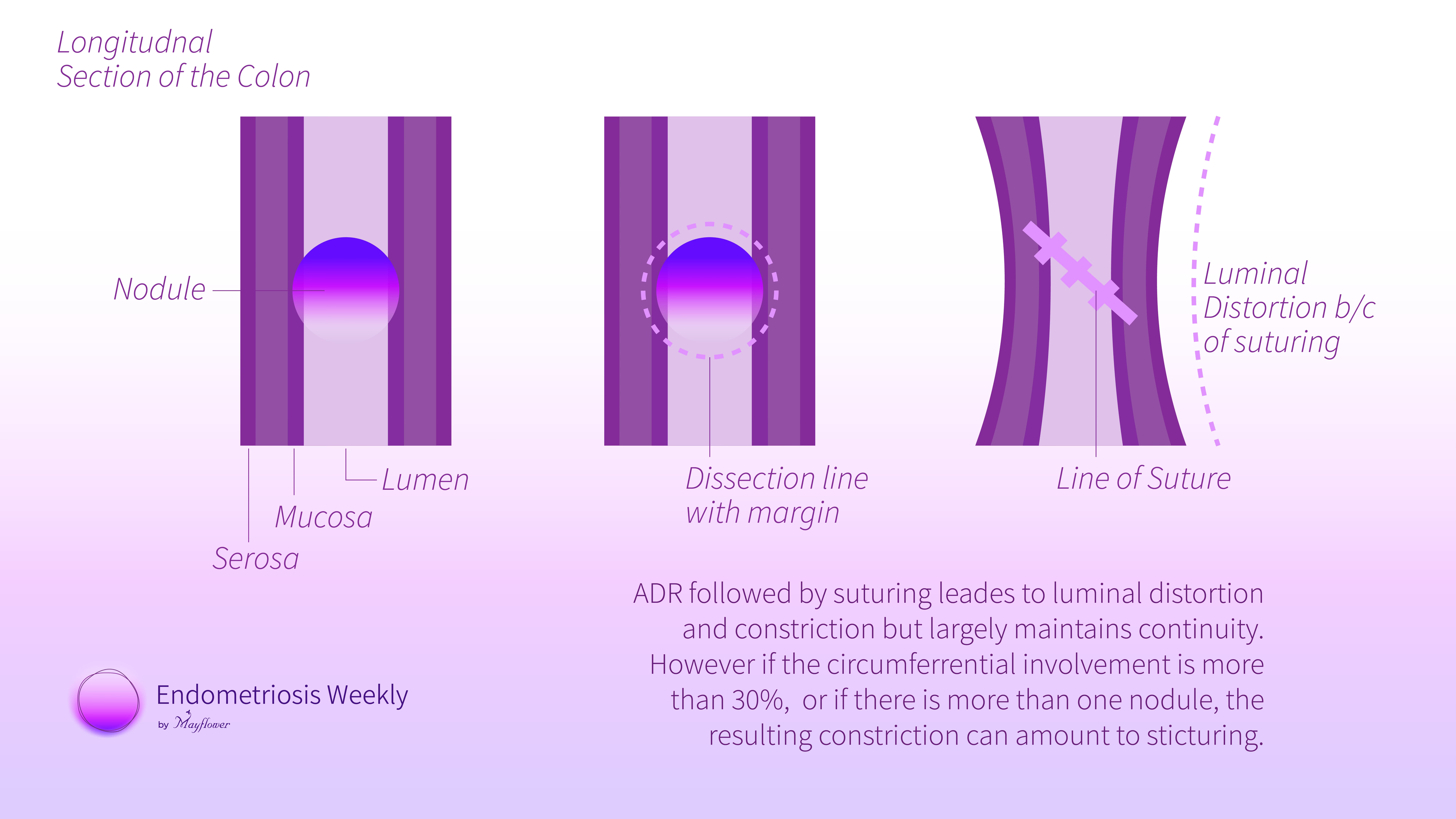
The rationale we used for explaining why the involvement must be less than 1/3rd of the circumference is the same as the rationale for a single nodule. So we can use the same diagram to illustrate it.
This is what makes triaging crucial. We don’t achieve anything by being conservative for anatomical preservation while leaving some disease behind. Conservatism becomes relevant when we begin removing too much for what it’s worth.
Cut Follows Cause
Remember that any dissection we perform, any aspect of the body that we distort or disturb, must follow some cause established for performing such an action. We must always ask ourselves why we are doing something, and what happens if we don’t.
For a better life for the patient, it is necessary that we remove the entirety of the disease. No compromise can be made there, or we almost certainly risk recurrence. But on the other hand, we cannot overcompensate and distort an already existing, well functioning, and docile anatomy without significant cause
Take this case for example. In this transverse section (axial) of the MRI we can see how there is a nodule (highlighted in green) invading the mucosa near the rectum.

Since it’s a single nodule and the circumferential involvement is less than 1/3rd, we can opt of ADR. The biggest benefit in this case is the preservation of neuro vascular continuity.
To start with, the rectum is mobilised from lateral to the medial side by entering the medial pararectal space and reaching upto the Denonvillers fascia from the lateral and medial side. Once the colon is free, we enter the Recto-vaginal plane and the rectum is freed from both the lateral and anterior sides to give it increased mobility. Mobility that helps us give the colon a tension free suturing which is the most important aspect in all bowel sutures.
We now jump right into the act. The first step is denudation of fat surrounding the nodule. Then for ADR, the nodule is firmly lifted.
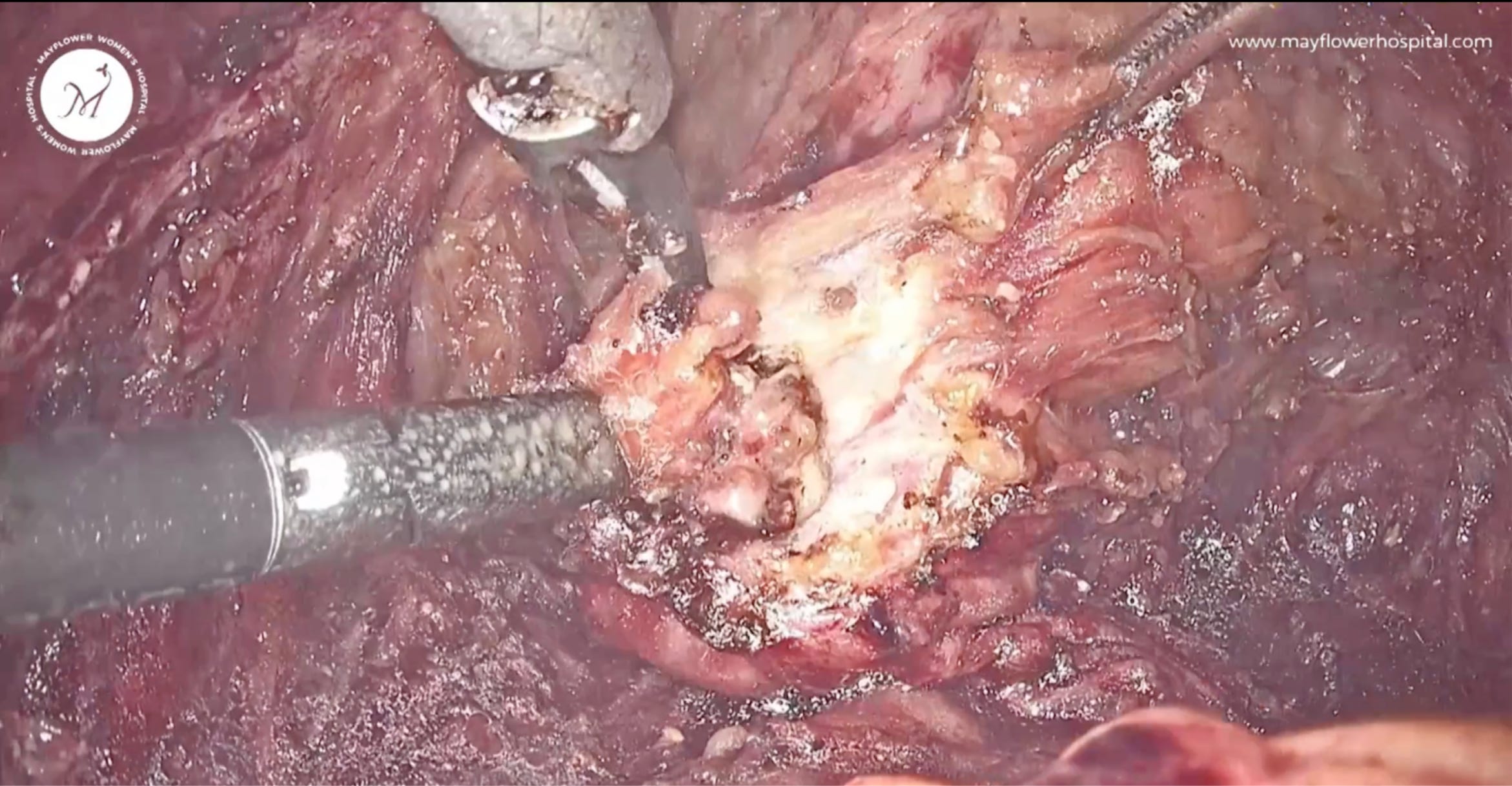
The involved anterior rectal wall carrying Endometriosis is resected. This dissection is always carried out in a fiber-by-fiber fashion. We first feel the nodularity, make sure the entire plaq is removed, and then conclude the dissection, ensuring we’ve left no diseased tissue behind.

Now, we begin closing the perforation. The first step is stay sutures, which are taken at the edges of the rent. This will also help us stabilise colon and prevent any further tearing of the rent.
We then follow it up by a rectal wall closure. It is done along the transverse line in 2 layers. We generally like to take the first layer in an interrupted manner with vicryl 3.0 and a second layer with v loc in continuous non locking or interrupted fashion - depending on the surgeon.

This is the final view of the closure. Note that this closure is also critical because it has to be both liquid as well as gas proof, ensuring there is no leakage of any digestive material into the pelvis.
And that’s ADR for you. A simple but effective procedure that can lead to a complete removal of an endometriotic nodule without causing a large part of the disruption that resection and anastomosis might have.
That’s the procedure. A lot of these images, videos, and transcripts are available to us thanks to the meticulous and engaged media editing team at Mayflower who go through all cases, and maintaining an elaborate archive of the surgeries we do. This also helps us give our patients a video of their procedure, even before their discharge.
Following the longest standing request from a lot of our fellow doctors, we’ve launched M Studios, a comprehensive surgery video editing service for professionally edited surgery videos, that are clear and complete with seamless transitions and annotations, edited by experts, all delivered in a quick turn around time.
If you wish to have your videos edited, please reach out to us. And if now, we will see you again next week.
 | A guest post by
|
 | A guest post by
|